










REPORT
May 2026
Read time: 21 min

This issue of McDermott Will & Schulte’s Healthcare Regulatory Check-Up highlights regulatory activity for April 2026, including recent enforcement actions involving the False Claims Act (FCA), two favorable Office of Inspector General (OIG) advisory opinions, and proposed and final rules issued by the Centers for Medicare & Medicaid Services (CMS). We also discuss OIG’s updates to its fraud and abuse frequently asked questions (FAQs) page, OIG’s report on CMS’s oversight of compounded drugs prescribed to Medicare beneficiaries, and OIG’s intent to publish reports on laboratory tests and GLP-1 drug compounding.
Click each heading below to view the newsletter content.
Stay up to date on the latest health regulatory developments. Subscribe to receive this newsletter directly in your inbox each month and never miss an update.










Healthcare Regulatory Check-Up Newsletter | March 2026 Recap
REPORT
April 2026
Read time: 4 min
This issue of McDermott Will & Schulte’s Healthcare Regulatory Check-Up highlights regulatory activity for March 2026, including three favorable Office of Inspector General (OIG) advisory opinions and the US Department of Health and Human Services’ (HHS’s) final rule adopting standards for healthcare claims attachments and electronic signatures. We also discuss the US Department of Justice’s (DOJ’s) recent antitrust suit against hospital systems; HHS and the Centers for Medicare & Medicaid Services’ (CMS’s) announcement of a new Healthcare Advisory Committee; and Florida’s implementation of a parallel Medicaid durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS) enrollment moratorium after CMS’s nationwide Medicare moratorium. This issue also covers recent enforcement activity involving antitrust actions, the False Claims Act (FCA), and suits involving the Health Resources and Services Administration (HRSA) and the US Food and Drug Administration (FDA).
Read below for an overview of this month’s regulatory and enforcement activity roundup. For a deeper dive, subscribe to the newsletter to get our detailed analysis of all updates.
Click each heading below for a sneak peek of related content.
Interested in reading the full newsletter? Sign up today and get a copy of the March 2026 Recap issue immediately.
Ashley Anumba, a law clerk in the New York office, also contributed to this newsletter.



Healthcare Regulatory Check-Up Newsletter | February 2026 Recap
REPORT
March 2026
Read time: 5 min
This issue of McDermott Will & Schulte’s Healthcare Regulatory Check-Up highlights regulatory activity for February 2026, including two False Claims Act (FCA) settlements, a new Office of Inspector General (OIG) advisory opinion, and the US Department of Health and Human Services’ (HHS’s) 2027 Notice of Benefit and Payment Parameters proposed rule. We also discuss recent actions from the Centers for Medicare & Medicaid Services (CMS), including the agency’s moratorium on certain Medicare durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS) supplier enrollments; the deferment of millions in Medicaid funding to Minnesota over fraud, waste, and abuse concerns; and the agency’s joint pledge with health plans to launch a new payment program aligned with CMS’s ACCESS model. This issue also covers recent activity by the Health Resources and Services Administration (HRSA) and the US Food and Drug Administration (FDA).
Read below for an overview of this month’s regulatory and enforcement activity roundup.
Click each heading below for a sneak peek of related content.
Interested in reading the full newsletter? Sign up today and get a copy of the February 2026 Recap issue immediately.




Healthcare Regulatory Check-Up Newsletter | January 2026 Recap
REPORT
February 2026
Read time: 6 min
This issue of McDermott Will & Schulte’s Healthcare Regulatory Check-Up highlights regulatory activity for January 2026. The US Department of Health and Human Services (HHS) Office of Inspector General (OIG) issued two advisory opinions and a special bulletin analyzing direct-to-consumer prescription drug platforms, including TrumpRx. The US Department of Justice (DOJ) issued two reports discussing enforcement activity in 2025. The Centers for Medicare & Medicaid Services (CMS) withdrew local coverage determinations for skin substitutes, released the Outpatient Prospective Payment System drug acquisition cost survey, introduced a new Innovation Center model, and published the advance notice of changes to calendar year (CY) 2027 Medicare Advantage (MA) and Part D rates. Several notable settlements also occurred in January, resulting from qui tam False Claims Act (FCA) investigations and civil cases.
Click each heading below for a sneak peek of related content.




A window into the latest EU and UK antitrust M&A activity: Clearance trends and CMA remedies
ARTICLE
February 2026
Read time: 6 min
The fourth quarter of 2025 underscored evolving merger control frameworks in the European Union and United Kingdom, marked by greater flexibility, streamlined processes, and pragmatic enforcement. Competition authorities are showing increased openness to behavioral remedies, encouraging deeper pre‑notification engagement, and prioritizing proportionate solutions that preserve pro‑competitive transactions. These developments highlight a regulatory environment in which strategic planning, early dialogue with authorities, and well‑crafted remedies are essential to securing timely approvals in both jurisdictions.
European Union
Early and close engagement with the Commission results in clearances
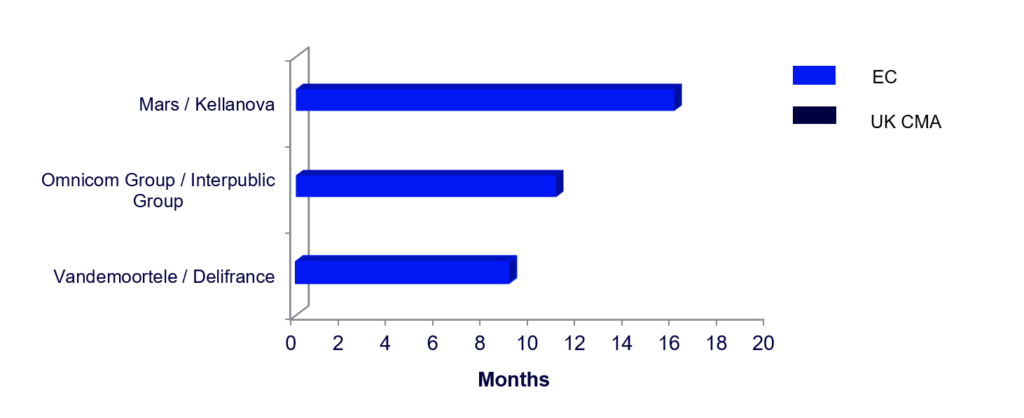
In the last quarter, the European Commission reviewed several complex transactions requiring significant regulatory scrutiny: (i) Mars’ acquisition of Kellanova, in which the Commission considered in-depth supplier power vis-à-vis supermarkets; and (ii) Omnicom’s acquisition of IPG, which was formally notified to the Commission in October 2024 and cleared in Phase 1, some 10 months after the deal was first announced.
In each case, the Commission eventually cleared the transaction, but only after requesting, reviewing, and considering thousands, if not hundreds of thousands, of documents submitted by the parties.
Unconditional clearance for Mars’ acquisition of Kellanova
One of the quarter’s most notable decisions saw the Commission unconditionally clear Mars’ acquisition of Kellanova in Phase 2 almost 16 months after deal announcement. The review focused on how the deal might affect bargaining dynamics with retailers for snack and cereal products. The Commission ultimately concluded that there was no credible risk of increased power leading to competitive harm, relying on the differentiated nature of the relevant product categories and the lack of evidence supporting increased brand loyalty or a “basket effect” on the part of consumers.
The investigation into portfolio effects highlights that the Commission will closely scrutinize transactions in markets where broad product portfolios play a large role and where products could be perceived as “must-stock.” Nevertheless, the unconditional clearance demonstrates that the Commission is unlikely to challenge under a portfolio effects theory without persuasive economic evidence and robust data.
Unconditional clearance for Omnicom’s acquisition of IPG
The Commission also unconditionally approved Omnicom’s acquisition of Interpublic Group (IPG), a merger that creates one of the world’s largest advertising and marketing services networks. The assessment found that existing competitive constraints – from players such as WPP, Publicis, and others – along with high customer mobility and relatively low switching costs, meant the deal was unlikely to significantly impede effective competition in the European Economic Area.
The parties did not formally file the transaction with the Commission until 10 months after deal announcement, after having obtained approval from multiple other jurisdictions. This transaction demonstrates that for complicated transactions parties need to spend a significant amount of time in pre-notification discussions with the Commission.
United Kingdom
CMA revises approach to remedies in year of streamlining merger control investigations
On December 19, 2025, the new guidelines for merger remedies, issued by the Competition and Markets Authority (CMA), took effect. The changes to the merger remedy guidelines are the latest installment in the CMA’s implementation of the “4Ps” framework – pace, predictability, proportionality, and process – which seeks to make merger control more transparent and business friendly. Key points include the following:
Behavioral remedies are more acceptable
While structural remedies remain the preferred option and the test remains the same (i.e., will the remedy be effective, and if so is the remedy proportionate?), the guidelines suggest a more open approach to behavioral remedies, especially if the CMA’s concern relates to specific activities and there is no other alternative remedy to “fix” an otherwise pro-competitive transaction.
Similarly, the CMA relaxed its position on accepting behavioral remedies during the first phase of the investigation. Behavioral remedies still must meet the “clear cut” standard, which requires that remedies must provide obvious and straightforward resolutions to competition concerns and be capable of ready implementation. However, the CMA highlights that early engagement on a remedy that aligns with established market practices and has a degree of market transparency, as well as the parties’ appointing a monitoring trustee, are all factors that increase the likelihood of the CMA accepting behavioral remedies early in the investigation.
Willingness to discuss remedies earlier in the review process
The CMA’s updated guidelines open the door for early, pre-notification discussions around remedies, with such discussions being “without prejudice” to the substantive analysis. Particularly with more-complex remedy packages that include carve-outs (as opposed to standalone businesses), the CMA seeks early engagement from the parties to provide measures to mitigate concerns such as the inclusion of an upfront buyer, the use of a monitoring trustee or independent expert to assess compliance, as well as potential alternative solutions should the remedy deal fall through.
The new guidelines bring to a close a year of realignment for the CMA and make the UK a much more deal-friendly environment.
After introducing new service standards that streamline the merger control process (reducing the average timeline from five to three-and-a-half months) and updating guidelines on jurisdiction and process, the CMA rounded out the year by publishing its latest annual merger investigation outcomes.
For calendar year 2025, the CMA considered 881 mergers (compared to 1,037 mergers in 2024), investigating 39 at phase 1 (compared to 38 in 2024), with only 4 referred to in-depth phase 2 review (compared to 6 in 2024). Of those phase 2 investigations, two were unconditionally cleared (compared to 2 in 2024), 1 resulted in acceptable remedies (compared to 2 in 2024), one was blocked (same as in 2024), and none was abandoned by the parties (compared to one in 2024). Overall, only 0.1% of all considered mergers were blocked or abandoned in 2025 (same as in in 2024).
EU and UK Q4 2025 M&A activity: By the numbers
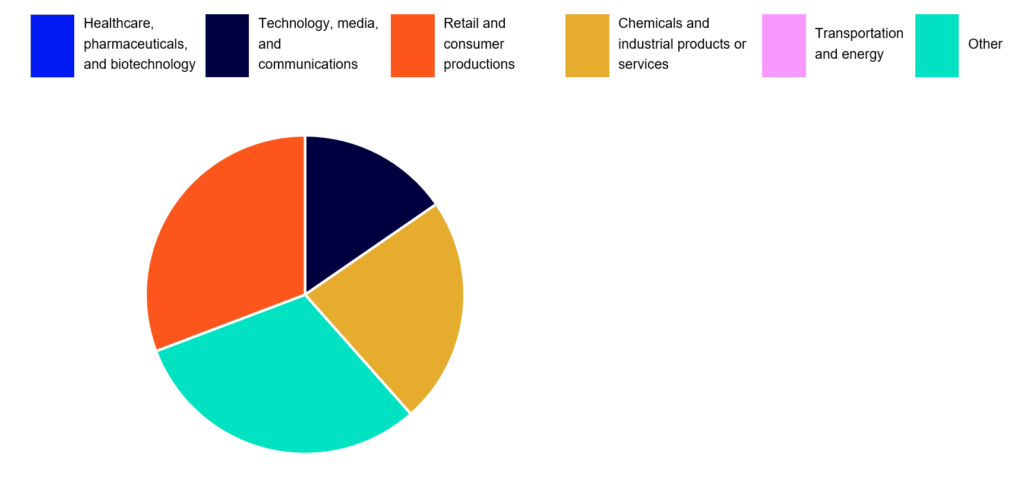
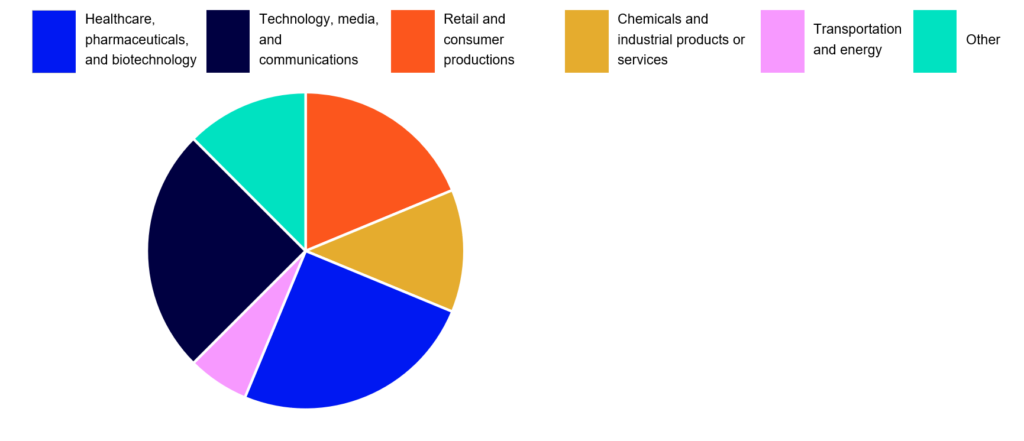
Number of enforcement actions in key industries1
Snapshot of selected enforcement actions2
Time from signing to clearance









5 lessons learned from US litigation wins/losses in 2025
ARTICLE
February 2026
Read time: 6 min
2025 proved to be a challenging year in court for the Federal Trade Commission (FTC), as it was unsuccessful in challenging the Tempur Sealy/Mattress Firm acquisition, the GTCR/Surmodics acquisition, a decade-old Meta Platforms acquisition, and (on appeal) the Microsoft/Activision Blizzard acquisition. These decisions provide several key takeaways for companies contemplating future M&A.
Overly aggressive, narrow product markets hurt the agencies’ claims
Courts have rejected relevant markets proposed by the FTC where the narrow segmentation is belied by the record and industry norms. In Tempur Sealy, the FTC alleged a “premium” market for mattresses over $2,000. The district court disagreed, finding competition for mattresses “fierce” and noting that the FTC’s own expert admitted that he picked $2,000 as a threshold merely because it gave Mattress Firm higher shares. In the retroactive challenge to Meta, the FTC’s proposed market included Facebook, Instagram, Snapchat, and MeWe but excluded YouTube and TikTok (which are not owned by Meta). The district court disagreed, finding that YouTube and TikTok were competitive substitutes to Facebook and Instagram. Ultimately, market definition is very fact dependent, and the agencies have won many cases by proving narrow markets where facts supported them, especially when business documents align with the narrow-alleged market. The FTC announced on January 20, 2026, that it will appeal the district court’s decision in Meta, and it remains unclear whether retroactive challenges — brought after market conditions have significantly changed since the original acquisition — will gain traction on appeal.
Courts are inclined to accept remedies as a fix to merger challenges
In Tempur Sealy and GTCR, the courts found that the merging parties’ proposed remedies mitigated any antitrust concerns. In GTCR, to address the horizontal overlap, the merging parties proposed a fix during the course of litigation to sell portions of GTCR’s Biocoat to Integer. In Tempur Sealy, to address vertical concerns, the judge found that behavioral remedies (e.g., slot commitments and supply agreements) and a small divestiture of stores undermined the FTC’s concerns. Similarly, in Microsoft, the court found that Microsoft’s licensing agreements and pledge to keep Activision’s key games on all platforms addressed the vertical foreclosure issues. Even when the regulators are unwilling to accept the proposed remedy, these cases demonstrate that courts are giving significant weight to remedies, enabling the parties to “litigate the fix” and prevail at trial.
Vertical challenges are hard to win
The courts have rejected vertical foreclosure theories of harm that rely solely on market share or a “big is bad” approach. In both the Microsoft/Activision Blizzard acquisition and the Tempur Sealy acquisition, the FTC failed to provide concrete evidence of likely foreclosure of competitors, post-acquisition. In Microsoft, the court found that Microsoft lacked profit incentives to only make games available on Microsoft’s gaming system, Xbox. In Tempur Sealy, in addition to the behavioral remedies offered, the court found the potential foreclosure harm for competitors was overstated, as Mattress Firm was not a critical sales channel for mattress manufacturers. While Mattress Firm was a large retail outlet, there were many other channels through which mattress suppliers could reach customers.
The FTC is moving away from in-house challenges
In its most recent transaction challenge, the FTC signalled a significant change in its enforcement practices, opting only to challenge the Henkel and A-Paint merger in federal court via a permanent injunction, rather than initiating an administrative action in parallel. Historically, the FTC has utilized Section 13(b) of the FTC Act, which allows the agency to seek a preliminary injunction in federal court where an administrative challenge is pending at the FTC. Under Section 13(b), a court can grant a preliminary injunction enjoining the merger until the case is heard in the administrative action if the FTC raises questions on the merits of the deal that are “serious, substantial, difficult and doubtful.” A permanent injunction, on the other hand, requires the FTC to succeed on the merits in proving that the merger may substantially lessen competition or tend to create a monopoly. While this change in practice means parties will only have to litigate one case at a time, the timeline for that challenge is likely to increase because of the additional legal and evidentiary standards that must be evaluated by the court. This change also aligns FTC antitrust enforcement more closely to that of the US Department of Justice (DOJ), which only utilizes a permanent injunction standard when challenging a merger.
Increased lobbying efforts in M&A prompts more state intervention
Twelve states and the District of Columbia have intervened in the latest settlement between the DOJ and merging parties, Hewlett Packard Enterprise (HPE) and Juniper Networks (Juniper). The HPE/Juniper settlement raised concerns after internal DOJ disagreements surrounding the deal became public, with former US Deputy Attorney General Roger Alford even calling the consent agreement “pay-to-play.” The intervening states have decried the settlement as the product of undue influence by well-connected lobbyists.
The publicity surrounding the settlement agreement has also called renewed attention to the Antitrust Procedures and Penalties Act (Tunney Act). Under the act, the DOJ must file proposed settlements in federal court for review, and the court evaluates the settlement agreement to see if it is in the public interest.
The states’ intervention in the HPE/Juniper settlement shows a pattern of increased state antitrust action amidst perceived politicized federal antitrust enforcement. Companies that are considering M&A activity should be cognizant that their lobbying efforts are likely to be monitored more closely, not just by the courts, but by state actors as well.
US Q4 2025 M&A activity: By the numbers
Number of enforcement actions in key industries1
Snapshot of selected enforcement actions2
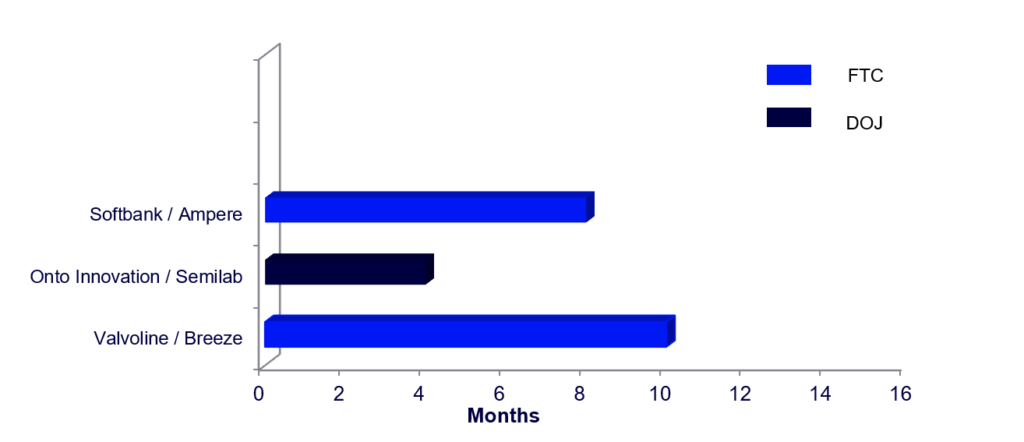
Time from signing to consent or investigation closing

Healthcare Regulatory Check-Up Newsletter | December 2025 Recap
REPORT
January 2026
Read time: 6 min
This issue of McDermott’s Healthcare Regulatory Check-Up highlights regulatory activity from December 2025. The end of the year brought a significant number of newly proposed Centers for Medicare & Medicaid Services (CMS) rules and Innovation Center models, as well as several new Office of the Inspector General (OIG) reports and an advisory opinion. We discuss enforcement actions focusing on allegations under the Anti-Kickback Statute (AKS), the False Claims Act (FCA), and other fraud and abuse laws, including allegations related to laboratory testing, wound grafts, and marketing schemes. This issue also discusses recent executive orders related to artificial intelligence (AI) and medical marijuana research.
Click each heading below for a sneak peek of related content.





Credit Conditions: The latest private credit and debt market trends | Q1 2026
REPORT
January 12, 2026
Read time: 2 min
Welcome to this edition of Credit Conditions, a quarterly publication that analyzes recent debt market trends.
End-of-year dealmaking accelerated across M&A, private equity, and credit markets, even as Federal Reserve uncertainty, tariffs, and shifting regulations pulled markets in competing directions. With renewed initial public offering exits, record loan repricings, and fierce competition between the broadly syndicated loan and private credit markets, Q1 sets the stage for a volatile but opportunity-rich 2026.
For more, access our Credit Conditions resource page.








Healthcare Regulatory Check-Up Newsletter | November 2025 Recap
REPORT
December 2025
Read time: 5 min
This issue of McDermott Will & Schulte’s Healthcare Regulatory Check-Up highlights regulatory activity for November 2025. Regulators are signaling clear priorities: stronger enforcement, modernization of compliance standards, and expanded access to care. Recent enforcement actions underscore risks tied to billing accuracy, kickbacks, and Emergency Medical Treatment and Labor Act (EMTALA) compliance. The Centers for Medicare & Medicaid Services (CMS) advanced sweeping updates, including telehealth extensions and hospital and ambulatory surgical center (ASC) payment reforms, and pursued cost-control initiatives such as drug price negotiations and new Medicaid rebate models. Providers should focus on compliance readiness, digital infrastructure, and strategic planning to navigate these changes effectively.
Click each heading below for a sneak peek of related content.




Healthcare Regulatory Check-Up Newsletter | October 2025 Recap
REPORT
November 2025
Read time: 4 min
This issue of McDermott’s Healthcare Regulatory Check-Up highlights regulatory activity for October 2025, which was relatively quiet due to the federal government shutdown. This month’s summary discusses revisions to the US Department of Health and Human Services (HHS) grants policy statement, the US Department of Education (DOE) public service loan forgiveness (PSLF) final rule, enforcement efforts and guidance from the US Food and Drug Administration (FDA) regarding biosimilars and weight loss drugs. We also review an Office of Inspector General (OIG) report regarding improper durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS) payments, and the latest developments in judicial invalidation of Biden-era nondiscrimination rules under Section 1557 of the Affordable Care Act (ACA). This issue examines the calendar year (CY) 2026 Physician Fee Schedule (PFS) from the Centers for Medicare & Medicaid Services (CMS), and CMS’s decision to lift claim holds that were in place during the shutdown because of expired Medicare payment provisions. We also discuss updates to the Advanced Medical Technology Association (AdvaMed) Code of Ethics, a recent California law regulating pharmacy benefit managers, and a HIPAA security risk assessment tool published by HHS.
Click each heading below for a sneak peek of related content.

