










CLIENT ALERT / INFORMATION BLOCKING
November 14, 2023
Read time: 11 min

On October 30, 2023, the US Department of Health and Human Services (HHS) Office of the National Coordinator for Health Information Technology (ONC) and the Centers for Medicare & Medicaid Services (CMS) released a long-awaited proposed rule to implement a 21st Century Cures Act provision establishing penalties (called “appropriate disincentives”) for health care providers determined by the HHS Office of Inspector General (OIG) to have committed information blocking. Health care providers have been subject to the information blocking regulations since April 5, 2021, but there has been no enforcement mechanism under the Cures Act to date.
KEY TAKEAWAYS
- While the HHS proposed rule moves the industry one step closer to enforcement of the information blocking regulations against health care providers, it would apply penalties only to health care providers that participate in certain Medicare programs and not to all health care providers that are covered actors under the information blocking regulations.
- HHS has not proposed any disincentives for health care providers that do not participate in the Medicare Promoting Interoperability or Medicare Shared Savings Program (MSSP), or that serve a limited number of Medicare beneficiaries.
- In a blog post accompanying the proposed rule, ONC was unequivocal about its position that “[i]nformation sharing is expected.” What remains unclear is the mechanics of how HHS will apply its proposed disincentives framework, and a close review of the proposed rule reveals several open questions.
- Comments on the proposed rule are due January 2, 2024.
For more information about ONC’s information blocking regulations, including who is a regulated actor, as well as important information blocking definitions and exceptions, see our Special Report. For a discussion of OIG’s final information blocking enforcement rule concerning the penalties for information blocking by health IT developers of certified health IT (certified health IT developers) and health information networks and health information exchanges (HIN/HIEs), plus OIG’s investigation and enforcement procedures, see our Special Report “A Million Reasons to Share: OIG’s Final Rule on Information Blocking Enforcement.”
SUMMARY OF PROPOSED DISINCENTIVES
The proposed rule would establish the following disincentives for certain Medicare-enrolled health care providers that OIG determines committed information blocking and referred to CMS. As discussed below, the ultimate financial impact of disincentives (if any) would vary in some instances based on Medicare reimbursement rather than on the severity of a health care provider’s alleged information blocking conduct or other factors related to interference with access, exchange or use of electronic health information (EHI). The proposed rule does not include disincentives for health care providers that are not enrolled in Medicare.
Hospitals and Critical Access Hospitals
HHS proposes to use the existing Medicare Promoting Interoperability Program for the meaningful use of certified electronic health record (EHR) technology to impose disincentives on eligible hospitals and critical access hospitals (CAHs). Under the proposed rule, an eligible hospital or CAH would not be a meaningful EHR user in an EHR reporting period if OIG refers, during the calendar year of the reporting period, its determination that the eligible hospital or CAH committed information blocking. As a result, a hospital would be unable to earn the three-quarters of the annual market basket increase, and a CAH would have its payment reduced to 100% of reasonable costs, down from 101%.
HHS estimates that this proposal could result in a median disincentive amount of $394,353 and a 95% range of $30,406 to $2,430,766. Of note, the Promoting Interoperability Program does not apply to many other facilities, laboratories, long-term care hospitals and other care sites.
Physicians and Other Clinicians Reimbursed Under the Medicare Physician Fee Schedule
With some exceptions, clinicians reimbursed under the Physician Fee Schedule (PFS) must either participate in a Medicare Advanced Alternative Payment Model (AAPM) or achieve a threshold Merit-based Incentive Payment System (MIPS) performance score to avoid a downward adjustment to their PFS reimbursement. CMS currently calculates the MIPS performance score based on four performance categories: Quality (30%), Improvement Activities (15%), Promoting Interoperability (25%) and Cost (30%). Measures within the four performance categories are scored and combined to make up a clinician’s MIPS final score. Those who score higher than a performance threshold set by CMS for a reporting year (75 points for 2024) can earn a positive adjustment of up to 9% of reimbursement under the PFS in the payment year. Likewise, those below the performance threshold face penalties of up to -9% of reimbursement under the PFS. CMS applies a payment adjustment to the payment year two years after the calendar year of the clinician’s MIPS reporting period. Not all MIPS participants are required to report the Promoting Interoperability category. For example, there are exceptions for facility-based and hospital-based clinicians (e.g., emergency room physicians and providers in ambulatory surgical centers) as well as some small practices.
Under the proposed rule, a clinician who participates in MIPS and is required to report on the Promoting Interoperability performance category would receive a zero score for the category if OIG refers, during the calendar year of the clinician’s reporting period, a determination that the clinician committed information blocking. Since the Promoting Interoperability performance category is currently 25% of the total MIPS score, 75 would be the highest score that the clinician could earn and would likely result in a penalty based on the current MIPS performance threshold for 2024. Those who do not report the MIPS Promoting Interoperability category would not be subject to any disincentives under this proposal.
HHS estimates that the median individual disincentive amount could be a loss of $686 for a clinician, while an estimated median group of six clinicians could see a loss of $4,116, with a range of $1,372 to $165,326 for group sizes ranging from two to 241 clinicians.
Medicare Shared Savings Program
Clinicians can avoid having to participate in MIPS, or can have their reporting requirements reduced, by participating in the Medicare Shared Savings Program (MSSP). CMS is moving to align certified EHR reporting requirements for all MSSP participants with those of the MIPS Promoting Interoperability performance category beginning in the 2025 performance year.
Because MSSP accountable care organizations (ACOs) are not yet required to report under the Promoting Interoperability program, CMS proposes a different disincentive in connection with the MSSP. Under the proposed disincentives rule, if OIG determines that a health care provider that is an ACO or part of an ACO has committed information blocking, that provider would be barred from participating in the MSSP for at least one year. This may result in a health care provider being removed from an ACO or prevented from joining an ACO. In the instance where a health care provider is an ACO, this would prevent the ACO’s participation in the MSSP.
SCOPE OF HEALTH CARE PROVIDERS IMPACTED BY PROPOSED DISINCENTIVES
The information blocking regulations apply to a broad range of health care providers, including facilities such as nursing facilities, long-term care facilities, dialysis facilities, blood centers, ambulatory surgical centers, laboratories and pharmacies, and individual providers such as therapists and pharmacists. However, because only a subset of health care providers is subject to the requirements that are the basis for disincentives under the proposed rule (e.g., the Promoting Interoperability requirements), many health care providers would be, at least initially, excluded from the disincentives framework, even though they are “covered actors” under the Cures Act and the information blocking regulations. In the proposed rule, HHS included a request for information on additional appropriate disincentives HHS should consider for future rulemaking efforts that would apply to the health care providers excluded from the disincentive framework in this rulemaking.
OIG INVESTIGATIVE AUTHORITIES, “REFERRALS” AND INTERSECTION WITH OIG CMP INFORMATION BLOCKING ENFORCEMENT RULE
The application of disincentives to health care providers covered by HHS’s proposal turns on a determination by OIG that the health care provider committed information blocking, so to understand the potential impact of HHS’s proposed rule, it is important to understand OIG’s role in the information blocking ecosystem.
The Cures Act granted OIG the authority to investigate information blocking claims against each type of covered actor—health care providers, certified health IT developers and HIN/HIEs. The Cures Act also granted OIG the authority to impose civil monetary penalties (CMP) against certified health IT developers and HIN/HIEs that violated the information blocking prohibition. OIG published its final rule implementing its CMP authority in the Federal Register in July 2023. That penalty authority, however, does not extend to the health care provider category of covered actors. Instead, the Cures Act requires OIG to refer health care providers that OIG determines have violated the information blocking prohibition to “the appropriate agency to be subject to appropriate disincentives.”
From a procedural perspective, the proposed rule notes that OIG will coordinate with the “appropriate agency” to which OIG plans to make a “referral” during the pendency of OIG’s investigation and before actually making the referral in an effort to ensure that the agency is aware that OIG might make the referral. When OIG actually does make the referral, OIG will provide information about its determination of information blocking, including how the health care provider’s practice met the “intent element” of the prohibition, among other data related to the alleged misconduct.
In the proposed rule, HHS identified OIG’s anticipated information blocking enforcement priorities for health care providers, which are identical to those OIG identified for certified health IT developers and HIN/HIEs except that OIG omitted actual knowledge from its enforcement priorities list for health care providers. This omission reflects the different knowledge standard in the statutory definition of information blocking for health care providers which must know that their alleged information blocking practice is likely to interfere with access, exchange or use of EHI to implicate the prohibition while health IT developers and HIN/HIEs must know or should know that their alleged information blocking practice is likely to interfere to implicate the prohibition.
In connection with OIG’s final rule, OIG provided guidance describing its planned investigative process for entities subject to information blocking CMPs. Interestingly, OIG stated in its final rule that its discussion of its anticipated enforcement priorities and investigative process was limited to those entities subject to CMPs, and not applicable to health care providers that may be referred for appropriate disincentives. Although the proposed rule discusses OIG’s enforcement priorities for health care providers, it largely omits discussion of the underlying investigative process, including whether OIG’s process will similarly include an opportunity for health care providers to discuss an OIG investigation and explain why their conduct either did not implicate the information blocking prohibition, met an exception or was otherwise lawful. This is notable given the absence in the proposed rule of any appeal mechanism by which health care providers could challenge OIG’s information blocking determination. Although there may be some limited opportunities to appeal a disincentive, HHS specifically makes clear that ACO appeals under the MSSP regulations, at least, do not extend to OIG’s underlying information blocking determination. HHS does not discuss any other appeal avenues in the proposed rule.
One would expect that OIG would need to engage with the health care provider to perform a reasonable investigation. But the OIG final rule’s disclaimer and the proposed rule’s omission of meaningful discussion about such interactions leaves open the question of what, if any, reasonable opportunities health care providers would have to make their case before being subjected to disincentives.
“WALL OF SHAME” FOR INFORMATION BLOCKING
The proposed rule would create a framework for public posts on ONC’s website about actors that OIG determines have committed information blocking. For health care providers subject to disincentives, the website would feature:
- The health care provider’s name;
- The provider’s business address (to ensure accurate provider identification);
- The practice found to have been information blocking; the disincentive(s) applied; and
- Where to find additional information, where publicly available, about the determination of information blocking.
HHS also proposes to post similar information on ONC’s website about HIN/HIEs and certified health IT developers that OIG determines have committed information blocking (regardless of whether they resolved their CMP liability with OIG or were subject to a CMP). The proposal is intended to provide transparency into how information blocking conduct is impacting the nationwide health information technology infrastructure.
This approach to transparency is similar to the HHS Office for Civil Rights’ notorious website that lists breaches of unsecured protected health information affecting 500 or more individuals (which is often referred to as the “wall of shame”). The transparency proposal is also an extension of the ONC’s existing website, Information Blocking Claims: By the Numbers, where it publishes statistics on the information blocking claims received through its “Report Information Blocking Portal” since April 5, 2021 (the information blocking compliance date). As of September 2023, ONC and OIG have received more than 800 claims of possible information blocking (including 685 claims against health care providers).
NEXT STEPS
If you would like to submit comments to the proposed rule before the January 2, 2024, deadline, contact any of the authors of this On the Subject or your regular McDermott lawyer or McDermott+Consulting advisor. Health care providers also should consider reviewing their information blocking policies and practices now so that they are ready for a future final rule.








ONC Extends Compliance Date for Information Blocking Rule
CLIENT ALERT / INFORMATION BLOCKING
November 17, 2020
Read time: 8 min
On November 4, 2020, the US Department of Health and Human Services Office of the National Coordinator for Health Information Technology (ONC) published an interim final rule with comment period in the Federal Register that extends certain compliance dates included in ONC’s May 1, 2020, final rule implementing the 21st Century Cures Act. Among other things, the ONC interim final rule pushed the compliance date for ONC’s information blocking provisions from November 2, 2020, to April 5, 2021. The interim final rule did not make substantive changes to the information blocking provisions or ONC’s Health IT Certification Program.
On November 4, 2020, the US Department of Health and Human Services Office of the National Coordinator for Health Information Technology (ONC) published an interim final rule with comment period (ONC IFR) in the Federal Register that extends certain compliance dates included in ONC’s final rule published in the Federal Register on May 1, 2020, to implement certain provisions of the 21st Century Cures Act. A key extension is the change of the information blocking prohibition applicability date (formerly, the “compliance date”) from November 2, 2020, to April 5, 2021. ONC also extended deadlines for certain health IT certification requirements included in the ONC final rule.
The ONC IFR did not establish penalties for information blocking by health care providers or make other substantive changes to the information blocking provisions of the ONC final rule or ONC’s Health IT Certification Program. (For more information regarding the substantive requirements of the ONC final rule, see our prior Special Report.) Rather, ONC stated that it is simply providing an extension in response to the unique circumstances of the Coronavirus (COVID-19) pandemic.
ONC recognized that the original compliance date did not allow sufficient time for covered actors, including certified health IT developers, health care providers and health information networks and health information exchanges (HIN/HIEs), to assess whether their arrangements and practices that involve the access, exchange or use of electronic health information (EHI) comply with the information blocking prohibition and, if appropriate, amend existing arrangements and implement new procedures to avoid information blocking, particularly when many covered actors are on the front lines combating COVID-19. ONC also concluded that certified health IT developers needed more time to update their software to address new requirements for application programming interfaces (APIs), EHI export and other capabilities.
Although appreciated, the ONC IFR—which spent more than a month under Office of Management and Budget review—came at the 11th hour, with many certified health IT developers and health care providers already well along the path of implementing their information blocking compliance strategies. Balancing against the need for resources to directly and indirectly combat the COVID-19 pandemic, certified health IT developers and health care providers can use the additional few months to test and refine information blocking prohibition compliance procedures. Specifically, health care providers should consider whether the additional time allows them to test or revisit their release of information practices or any plans for the availability of EHI through their patient portals. Similarly, certified health IT developers should evaluate whether the extension to the health IT certification criteria deadlines affect their software development timelines.
Stakeholders may submit comments to the ONC IFR through 5 pm EST on January 4, 2021.
The following sections discuss the new compliance dates applicable to (1) certified health IT developers, HIN/HIEs and health care providers, and (2) only certified health IT developers under the ONC’s Health IT Certification Program.
Changes to Key Compliance Dates Applicable to Certified Health IT Developers, HIN/HIEs and Health Care Providers
April 5, 2021
- Information Blocking Provisions
ONC extended the applicability date for the information blocking prohibition from November 2, 2020, to April 5, 2021. The information blocking provisions prohibit practices that the actor knows are likely to interfere with access, exchange or use of EHI, unless the practices are required by law or are covered by one of the eight exceptions established by ONC. For health care providers, the provider must also know that the practice is unreasonable for it to constitute prohibited information blocking. For the first 18 months, the information blocking provisions will only apply to EHI identified by the data elements represented in the US Core Data for Interoperability (USCDI).
October 6, 2022
- Scope of Information Blocking Provisions Expands to the Full Electronic Designated Record Set
ONC changed the date on which the scope of the information blocking provisions expands from the data elements represented in the USCDI to the full electronic designated record set as defined in the HIPAA regulations from May 2, 2022, to October 6, 2022.
Changes to Key Dates Applicable Only to Certified Health IT Developers
April 5, 2021
The ONC IFR extended the compliance date for the following health IT certification requirements applicable to certified health IT developers from November 2, 2020, to April 5, 2021.
- Information Blocking Condition of Certification (CoC) requirement
The Information Blocking CoC provides that a certified health IT developer must not engage in practices that constitute information blocking. Thus, in addition to potential civil monetary penalties for information blocking under the Cures Act, a certified health IT developer may jeopardize its products’ certification status if it engages in information blocking. The April 5, 2021, compliance date for the CoC aligns it with the new applicability date for the ONC final rule’s separate information blocking provisions.
- Assurances CoC and Maintenance of Certification (MoC) requirements
The ONC final rule’s Assurances CoC requires certified health IT developers to provide satisfactory assurances that they will not take any action that constitutes information blocking, and will ensure that their health IT conforms to the full scope of the certification criteria. The Assurances MoC requires certified health IT developers to retain all records and information necessary to demonstrate initial and ongoing compliance for 10 years beginning from the date the developer’s health IT is first certified.
- API CoC – compliance for current API criteria
The ONC final rule’s API CoC requires health IT developers that offer certified APIs to allow EHI to be accessed, exchanged and used through the certified API without special effort, and to publish complete business and technical documentation via a publicly accessible hyperlink that allows any person to directly access the information without any preconditions or additional steps. The CoC also establishes specific limitations to fees, terms and conditions that certified health IT developers may apply to their certified APIs.
- Communications CoC/MoC requirements
The Communications CoC provides that a certified health IT developer must not prohibit or restrict communications regarding the usability, interoperability or security of its health IT; the developer’s business practices; or the manner in which someone has used the developer’s health IT. Until developers have revised their contracts with customers and other contractors in accordance with the CoC, the Communications MoC requires developers to issue an annual written notice to the customers and contractors stating that they may make communications on these topics, even if the customer has agreed to contract provisions that contradict the CoC and would otherwise prohibit such communications.
December 15, 2021
- Submission of initial plan for real world testing
The ONC final rule requires certified health IT developers to submit testing plans to their certifying bodies to test a subset of certified health IT functionality in the setting(s) where the certified health IT modules are (or will be) marketed.
April 1, 2022
- Submission of initial attestations
Certified health IT developers are required to attest on a semiannual basis beginning on April 1, 2022, that they are in compliance with applicable CoC and MoC requirements.
December 31, 2022
The ONC IFR extends the deadline for certified health IT developers to update their software to include certain new certified capabilities from May 2, 2022, to December 31, 2022:
- New standardized API functionality
Certified health IT developers with certified APIs are required to make available FHIR-based APIs certified to § 170.315(g)(10) by no later than December 31, 2022.
- 2015 Edition health IT certification criteria updates in the ONC final rule (except for the updated EHI export capability, which is extended until December 31, 2023)
Certified health IT developers must update health IT modules certified to various other 2015 edition certification criteria to address revised standards and specifications established under the ONC final rule.
March 15, 2023
- Submission of initial results of real-world testing
The ONC final rule requires certified health IT developers to submit the results of real-world testing of each of their certified health IT modules to their certifying bodies each calendar year. The ONC IFR provides that the first real-world testing results report is not due until March 15, 2023.
December 31, 2023
- EHI export capability must be made available
The ONC final rule requires certified health IT developers of health IT modules that are part of a product that electronically stores EHI to provide customers with the ability to export EHI from the product in accordance with a new EHI export certification criterion. This criterion includes the ability to export the EHI of both a single patient and the entire patient population.
* * *
In conjunction with the release of the ONC IFR, ONC also issued Frequently Asked Questions on its website. Certified health IT developers and other actors regulated under the ONC final rule should review the Frequently Asked Questions and work with counsel to evaluate whether the guidance affects stakeholders’ approaches to information blocking compliance.
Please do not hesitate to contact your regular McDermott lawyer or any of the authors of this On the Subject if you have questions about or need assistance implementing compliance with the ONC final rule or its extended compliance dates.

Information Blocking Considerations for Health Systems Offering EHR System Access to Community Physicians and Facilitating Health Information Exchange
CLIENT ALERT / INFORMATION BLOCKING / INTEROPERABILITY
October 9, 2020
Read time: 3 min
On September 17, 2020, the Office of Management and Budget received an Interim Final Rule for review from the Office of the National Coordinator for Health IT (ONC) entitled “Information Blocking and the ONC Health IT Certification Program: Extension of Compliance Dates and Timeframes in Response to the COVID-19 Public Health Emergency.” While the title suggests that health care providers and other regulated actors may have more time to come into compliance with ONC’s May 2020 information blocking final rule, details about potential delays remain scarce and health care providers would be well served to continue apace with compliance efforts, even if the original November 2, 2020 information blocking compliance date ultimately shifts.
This is particularly true for hospitals and health systems that might also function in the capacity of a health information technology (IT) developer of certified health IT (Certified Health IT Developer) or health information network or health information exchange (HIN/HIE), because Certified Health IT Developers and HIN/HIEs face potential civil monetary penalties (CMPs) from the HHS Office of Inspector General (OIG)—as opposed to the yet undefined “appropriate disincentives” health care providers face. OIG is currently engaged in its own rulemaking to finalize regulations implementing its information blocking CMP authorities. In its proposed rule, OIG stated that it would not enforce CMPs for violations of the information blocking regulations that occur after November 2, 2020, but before OIG finalizes the CMPs. It is not clear how, if at all, any change to the ONC’s information blocking compliance date would impact the timing of OIG’s final rule (which is not yet at OMB for review) and, ultimately, timing of enforcement actions. Given such uncertainty, continued effort to identify and address areas of potential non-compliance with ONC’s final rule is advisable, particularly for actors that face potential CMPs of up to $1M per violation. For more information on the OIG proposed rule, see our On the Subject.
To help health care providers that might also function as Certified Health IT Developers or HIN/HIEs identify potential areas of consideration and focus, we have developed the below resources. Please reach out to your McDermott lawyer or one of the contacts listed here to discuss your information blocking preparations.
Additional Resources
October 13 Webinar with The Chartis Group | APIs and Information Blocking: What Providers Need to Know
REGISTER

Could Offering EHR System Access to Community Providers Lead to Civil Monetary Penalties for Information Blocking?
CLIENT ALERT / INFORMATION BLOCKING
June 17, 2020
Read time: 11 min
Under the Office of the National Coordinator for Health IT (ONC) 21st Century Cures Act final rule, effective July 1, 2020, health care providers, in their capacities as such, are not subject to information blocking civil monetary penalties. However, health systems, hospitals and other health care providers may face information blocking civil monetary penalties if they engage in activities that cause them to be a health information technology (IT) developer of certified health IT (Certified Health IT Developer) or health information network or health information exchange (HIN/HIE), and engage in activities that are “likely to interfere” with the access, exchange or use of electronic health information (EHI). This On the Subject discusses whether a health system or provider could be a Certified Health IT Developer or an HIN/HIE when it provides access to its electronic health record (EHR) system to unaffiliated community providers, and the potential risk that EHR access terms or practices could subject the health system or provider to civil monetary penalties for information blocking.
A hospital or other health care provider is an actor subject to the new information blocking restrictions under the final rule issued by the ONC under the 21st Century Cures Act (Final Rule), but is not subject to information blocking civil monetary penalties unless it (1) is a Certified Health IT Developer (including as an offeror of certified health IT), or (2) operates an HIN/HIE in which more than two unaffiliated parties access, exchange or use EHI.
The software license agreements between many certified EHR vendors and their health system or other health care provider customer-licensees (EHR System Licensees) allow the EHR System Licensees to offer EHR system access to non-employed physician practices and other unaffiliated community providers for implementation and use in their physician office locations and other facilities. The EHR System Licensees typically provide access to their EHR systems as part of an agreement structured to meet the Stark Law exception and/or the federal anti-kickback statute safe harbor for EHR items and services, or waivers available under certain accountable care and other value-based care models. When the EHR System Licensee, its affiliated providers and community providers share an instance of the EHR system, they are able to access, exchange and use EHI created by any of the EHR system users, including the unaffiliated community providers. The offering of these EHR access arrangements may cause the EHR System Licensee to meet the definition of a Certified Health IT Developer and/or an HIN/HIE. We discuss this risk below. For more information about the Final Rule, please see our Special Report.
Certified Health IT Developers
The following sections address the Final Rule’s definition of a Certified Health IT Developer and questions that an EHR System Licensee should consider when evaluating whether an EHR access agreement could cause it to be Certified Health IT Developer.
What Is a Certified Health IT Developer?
The Final Rule defines a Certified Health IT Developer as follows:
- An individual or entity, other than a health care provider that self develops health IT for its own use, that develops or offers health information technology and which has, at the time it engages in a practice that is the subject of an information blocking claim, one or more Health IT Modules certified . . . pursuant to [the] ONC Health IT Certification Program…. (emphasis added)
The Final Rule does not clarify who is an “offeror” or what offeror activities would constitute “information blocking.” The Final Rule also fails to explain what it means for an offeror to “[have], at the time it engages in a practice that is the subject of an information blocking claim, one or more Health IT Modules certified . . . pursuant to [the] ONC Health IT Certification Program.”
An EHR System Licensee that is not the EHR vendor that sought and obtained the certification for the EHR software under the ONC Health IT Certification Program does not seem to “have . . . one or more Health IT Modules certified” and therefore arguably could never meet the definition of a Certified Health IT Developer. However, ONC’s preamble discussion of the definition is not clear on this point, and until ONC resolves the ambiguity, an EHR System Licensee that offers EHR system access to community providers should consider whether any of its EHR access agreement terms or other practices involving the access, exchange or use of EHI with community providers in connection with such agreements could constitute information blocking.
Is the EHR System Licensee a Certified Health IT Developer?
To assess whether an EHR System Licensee could be a Certified Health IT Developer, the EHR System Licensee should consider the following questions related to an offer of access to certified EHR technology to community providers:
- Does the EHR System Licensee simply make portions of payments to an EHR vendor to enable community providers to license a separate instance of the EHR software (or other certified health IT) directly from an EHR vendor?
- If so, then the EHR System Licensee may not be considered an “offeror” within the definition of a Certified Health IT Developer since the EHR vendor licenses the software directly to the community providers.
- Does the EHR System Licensee offer to enter into an agreement with community providers under which community provider personnel may access and use the EHR System Licensee’s instance of the EHR system in the community provider’s offices or other facilities?
- If the EHR System Licensee offers access to its EHR system, then the EHR System Licensee may be considered a Certified Health IT Developer based on the “offer.”
HINs and HIEs
The following sections discuss the Final Rule’s definition of an HIN/HIE, and questions that an EHR System Licensee should consider when evaluating whether an EHR access agreement could cause it to be an HIN/HIE.
What Is an HIN/HIE?
The Final Rule combines the definitions for HIN and HIE into one definition as follows:
- An individual or entity that determines, controls or has the discretion to administer any requirement, policy or agreement that permits, enables or requires the use of any technology or services for access, exchange or use of EHI:
- Among more than two unaffiliated individuals or entities (other than the individual or entity to which this definition might apply) that are enabled to exchange with each other; and
- That is for a Treatment, Payment or Health Care Operations purpose, as such terms are defined in the HIPAA regulations, regardless of whether such individuals or entities are subject to the HIPAA regulations.
An EHR System Licensee should evaluate whether its implementation of EHR access agreements to facilitate the exchange of EHI by or with community providers meets the above definition. For example, EHR System Licensees that provide EHR system access to community providers may implement security safeguards or procedures to control the flow of EHI among the community providers through the EHR system. The exercise of such control, even if to serve a legitimate privacy function that is not information blocking (e.g., preventing a community provider from accessing the EHI of non-patients in violation of HIPAA), could in turn cause the EHR System Licensees to meet the definition of an HIN/HIE.
Is the EHR System Licensee an HIN/HIE?
To assess whether an EHR System Licensee could be considered an HIN/HIE, the EHR System Licensee should consider the following questions:
- Does the EHR System Licensee administer or control any policy, agreement or requirement that permits, enables or requires the use of technology (e.g., health information exchange functionality) that enables the exchange of EHI among more than two unaffiliated individuals or entities (not counting the EHR System Licensee)?
- If the EHR System Licensee administers access to technology that enables more than two unaffiliated individuals or entities to exchange EHI, then is the exchange for Treatment, Payment or Health Care Operations (as each term is defined by the HIPAA regulations)?
- For example, can the unaffiliated entities use the technology to exchange EHI with each other to coordinate the care they provide to a common patient? If yes, then the EHR System Licensee may be considered an HIN/HIE.
What Practices in Connection with Health IT Access Arrangements Raise Potential Information Blocking Concerns?
If the EHR System Licensee is a Certified Health IT Developer (as an offeror) or an HIN/HIE, then the EHR System Licensee should structure its agreements with community providers consistent with the information blocking exceptions under the Final Rule to avoid the risk of information blocking civil monetary penalties. For example, the EHR System Licensee should consider the following questions:
- If an EHR System Licensee is a Certified Health IT Developer:
- Does the EHR System Licensee host (in its data center or through a third party) the EHI created by or received on behalf of the community providers?
- If the EHR System Licensee hosts the EHI, it could be in a position to exercise control over the EHI in ways that could implicate the information blocking prohibition.
- Even if the EHR vendor hosts the EHR system and EHI, the EHR System Licensee may still be in a position to exercise control over the EHI (e.g., through its control of EHR system configuration settings) in ways that could implicate the information blocking prohibition.
- Does the EHR System Licensee actually exercise control over some or all of the EHI created or received by the community provider in the certified health IT? For example, does the EHR System Licensee control the EHR system configuration settings that determine whether a particular user may access EHI in the EHR system?
- Under the Final Rule preamble, ONC stated that an offeror could be subject to the information blocking prohibition with respect to EHI it “hold[s] or control[s].” If an EHR vendor holds or controls providers’ EHI, then an EHR System Licensee that is a Certified Health IT Developer because it offers access rights to community providers, but does not hold or control the EHI, would not, under ONC’s preamble discussion, seem to be in a position to engage in information blocking in its capacity as an offeror. Further, under a specific Cures Act provision, the EHR System Licensee would not be responsible for actions taken by the EHR vendor that could constitute information blocking.
- Does the EHR System Licensee host (in its data center or through a third party) the EHI created by or received on behalf of the community providers?
- Does the EHR System Licensee condition access to the EHR system (including, for example, its HIN/HIE functionality) on the community provider’s provision of intellectual property rights?
- If yes, does the practice comply with the Final Rule’s Content and Manner Exception, Fees Exception or Licensing Exception? Note that under the Licensing Exception, actors may not require licensees or sublicensees (e.g., the community provider) to grant, assign or transfer to the actor any intellectual property of the licensee in return for the license or sublicense.
- Does the EHR System Licensee’s EHR access agreement with a community provider address the disposition of records maintained within the EHR upon termination of the agreement?
- Termination provisions that limit the community provider’s access, exchange or use of EHI post-termination could implicate the information blocking prohibition. (Likewise, a provision requested by the community provider that limits the EHR System Licensee’s access to the EHI may implicate the information blocking prohibition, since health care providers are subject to the prohibition. However, even if the community provider’s practice constitutes information blocking, it would not subject the community provider to civil monetary penalties because the community provider would be acting as a health care provider and not a Certified Health IT Developer or an HIN/HIE.)
- Does the EHR System Licensee control the timing and implementation of bug fixes, upgrades and other software maintenance to the EHR system (including its HIN/HIE functionality)?
- The Health IT Performance Exception permits actors in certain circumstances to inhibit the access, exchange or use of EHI for a limited period of time to perform planned or unplanned maintenance or updates. To comply with this exception, EHR System Licensees that control the timing and implementation of software maintenance or upgrades that could slow or cut off access to EHI should consider including service level agreement terms that establish a framework for limited planned and unplanned periods of maintenance in the EHR access agreement.
These are just some of the questions that health systems, hospitals and other health care providers potentially meeting the definition of a Certified Health IT Developer or an HIN/HIE should consider to ensure that they structure their EHR access agreements and conform their related practices in ways that mitigate potential information blocking civil monetary penalty exposure under the Final Rule.
Please contact your regular McDermott lawyer or any of the authors of this On the Subject if you have questions or need assistance with your compliance obligations under the Final Rule.

ONC and CMS Delay Enforcement Dates for Certain Provisions of the 21st Century Cures and Interoperability Final Rules, and OIG Announces Proposed Rule to Implement Information Blocking Enforcement Authority
CLIENT ALERT / INFORMATION BLOCKING
April 23, 2020
Read time: 9 min
On April 21, 2020, the US Department of Health and Human Services (HHS) Office of the National Coordinator for Health Information Technology (ONC) and Centers for Medicare & Medicaid Services (CMS) announced that they will exercise discretion to delay enforcement of certain provisions of their final information blocking and interoperability rules beyond the compliance dates established by these rules. In addition, the HHS Office of Inspector General (OIG) announced a proposed rule amending its civil monetary penalty (CMP) regulations to incorporate new CMP authorities for information blocking.
The Office of the National Coordinator for Health Information Technology (ONC) and the Centers for Medicare & Medicaid Services (CMS) first displayed the contents of their information blocking and interoperability final rules on March 9, 2020. Those rules contained various compliance dates for new requirements that were tied to the publication date of the final rules in the Federal Register. After initially delaying the compliance dates by withholding the final rules from publication in the wake of the Coronavirus (COVID-19) public health emergency, the agencies have now announced that the final rules will be published in the Federal Register on May 1, 2020. ONC and CMS will then exercise discretion to delay enforcement of certain provisions beyond the compliance dates published in the final rules in recognition of the health care industry’s current focus on the ongoing COVID-19 public health emergency.
Importantly, the enforcement delays announced by ONC and CMS do not affect the substantive requirements of the final rules. For more information on the substance of the final rules, please see our Special Alert and our other On The Subjects here and here.
In this On The Subject, we discuss the new compliance dates of the ONC and CMS final rule requirements and review OIG’s proposed amendments to the CMP rules.
ONC Final Rule
ONC announced that it will exercise its discretion and not enforce the new certification requirements of its final rule until three months after each compliance date or timeframe identified in the ONC final rule. Along with the announcement, ONC published a helpful table outlining the compliance timeframes for each of these provisions and the effect of the enforcement delay. ONC did not extend the compliance date for the information blocking provisions of its final rule, but as discussed below OIG’s rulemaking will determine the timing of enforcement activity. Below, we provide the key compliance dates based on the enforcement delays announced by ONC:
- ONC will begin enforcing two of the new conditions of certification (CoCs) on September 30, 2020 (three months from the June 30, 2020, compliance date in the final rule):
- Under the final rule, certified health IT developers may only prohibit or restrict communications by its customers about certified health IT under limited exceptions intended to allow the developer to reasonably protect its intellectual property. While developers must adhere to this CoC beginning September 30, 2020, they will have until March 31, 2021, to provide the required notice for the 2020 calendar year to customers stating that non-compliant confidentiality provisions or other restrictions or limitations on communications in existing contracts between the developer and the customer are invalid.
- Certified health IT developers must ensure that their certified health IT conforms to the full scope of the certification criteria applicable to the developer, and that the developer has not taken any action to interfere with a user’s ability to access or use certified capabilities.
- ONC will enforce the following CoCs on February 1, 2021 (three months after the November 1, 2021, compliance date for these provisions in the final rule):
- Certified health IT developers may not take any action that constitutes information blocking under the final rule.
- Certified application programming interface (API) developers must meet the CoCs relating to API transparency (publicly publishing business and technical documentation), charge only permissible API fees and offer APIs on open and pro-competitive terms.
- ONC will enforce the following CoCs on August 1, 2022 (three months after the May 1, 2022, compliance date for these provisions under the final rule):
- Certified health IT developers with currently certified APIs must meet the new API certification criteria, which includes implementation of the Fast Healthcare Interoperability Resources (FHIR) standard.
- Certified health IT developers will by this date need to have updated their products to comply with the United States Core Data for Interoperability (USCDI) criteria.
- Certified health IT developers must submit initial plans for real-world testing to their certification bodies so that their certification bodies may evaluate the plan’s completeness and submit the plan to the ONC’s Certified Health IT Product List (CHPL) by March 15, 2021 (three months from the December 15, 2020 compliance date in the final rule). Certification bodies will be required to post certified health IT developers’ real-world testing results to the CHPL by June 15, 2022 (three months from the March 15, 2022, compliance date in the final rule).
- Certified health IT developers will be required to submit their initial attestation that they adhered to the CoCs effective during the period of September 30, 2020 – March 31, 2021 by July 30, 2021.
- Developers must meet the new electronic health information (EHI) export certification criterion by August 1, 2023 (three months after the May 1, 2023, compliance date under the final rule).
CMS Interoperability Final Rule
The CMS final rule requires Medicare Advantage plans, Medicaid state agencies, Medicaid managed care plans, CHIP agencies, CHIP managed care entities, and issuers of qualified health plans on federally-facilitated exchanges (Covered Plans and Agencies) to implement APIs that allow patient information to be shared more readily with third-party applications selected by patients. The new API requirement for Covered Plans and Agencies was scheduled to go into effect on January 1, 2021. However, CMS announced it will exercise enforcement discretion for the API requirement for a period of six months until July 1, 2021.
Notably, however, CMS announced that all other policies in the final rule concerning Covered Plans and Agencies will be implemented and enforced on schedule. Covered Plans and Agencies will therefore still be expected by January 1, 2022, to have the ability to, in response to a patient’s request, forward patient information electronically to other payors designated by a requesting patient for up to five years after the patient has disenrolled from the plan.
The CMS final rule also requires Medicare hospitals that have adopted electronic health record systems to, as a condition of participation (CoP) in the Medicare program, electronically report patient admissions, discharges, and transfers to patients’ primary care practitioners or other practitioners primarily responsible for the patient’s care. Originally, the final rule made the new CoP effective for hospitals six months following publication of the final rule. However, CMS announced that it has changed the text of the final rule to state that the CoP will now be effective May 1, 2021 (12 months after the final rule’s publication).
OIG Proposed CMP Rule Amendments
On April 21, 2020, OIG released a proposed rule amending its civil monetary penalty (CMP) regulations. Among other things, OIG’s proposed rule would incorporate statutory changes, including those related to new CMP authorities for information blocking, into OIG’s existing CMP regulations. OIG states that it intends for the proposed information blocking enforcement regulations to “improve coordination within the health care system and patients’ access to their health care data.”
Enforcement Timing
Consistent with ONC’s discussion in the preamble to its final rule, OIG states that it will not begin CMP enforcement before ONC’s information blocking compliance date (November 1, 2020). OIG also proposes that, in any event, it will not begin enforcement until at least 60 days after OIG issues a final rule. Conduct occurring between ONC’s compliance date and OIG’s effective date—if ONC’s compliance date occurs first—will not be subject to CMPs. Of note though, OIG is considering an alternative proposal that would establish an effective date on a date certain. OIG identifies October 1, 2020, as a date under consideration, but is also considering earlier or later dates. OIG is seeking comment on when it should begin enforcement and how various considerations, including the ongoing COVID-19 pandemic, should affect information blocking enforcement timing.
OIG Enforcement Priorities
OIG states that its proposed rule does not include new information blocking requirements, but instead seeks to formally incorporate ONC’s information blocking regulations as the basis for OIG imposing information blocking CMPs. OIG does, however, provide examples of how it plans to determine whether an actor’s practice resulted in one or many information blocking violations, which is relevant to determining the amount of potential penalties and is an area where the regulated industry is likely to have a significant interest in providing feedback.
Like other OIG authorities that include an intent element, OIG acknowledges that each information blocking allegation will require a facts and circumstances analysis, which OIG will conduct in coordination with ONC and the HHS Office for Civil Rights. In terms of enforcement priorities, OIG states that it will focus on investigating conduct that (1) involves patient harm; (2) impacts providers’ ability to deliver patient care; (3) continues for a long time; (4) results in financial loss for Medicare, Medicaid, and other federal health care programs as well as other government and private entities; and (5) involves an actor engaging in the conduct with “actual knowledge.”
The last focus area is noteworthy because the 21st Century Cures Act provides for CMPs to be issued in situations in which health IT developers, health information exchanges and health information networks “know” or “should know” that their practices are likely to interfere with the access, exchange or use of EHI. OIG seems to be saying that it plans to focus on a subset of conduct that it could otherwise pursue for CMPs. That said, OIG goes out of its way in the proposed rule to note that the stated priorities in the preamble guidance will not legally restrict OIG’s discretion to choose the complaints it investigates.
Public Comment
OIG seeks public comment on its proposed rule. Interested stakeholders will have 60 days from the date of the proposed rule’s publication in the Federal Register to submit comments, though OIG stated that it will monitor requests for an extended comment period due to the COVID-19 public health emergency. The proposed rule is scheduled for publication on April 24, 2020.
Please do not hesitate to contact your regular McDermott lawyer or any of the authors of this On The Subject if you have questions or need assistance with your compliance obligations under the ONC/CMS final rules or if you have questions or wish to comment on the OIG proposed rule.

Analyzing Fee Restrictions for Health IT and EHI Under ONC’s Final Information Blocking Rule
CLIENT ALERT / INFORMATION BLOCKING / INTEROPERABILITY
March 20, 2020
Read time: 21 min
The Office of the National Coordinator for Health Information Technology recently released a final rule under the 21st Century Cures Act to promote interoperability of health IT and advance access, exchange or use of electronic health information (EHI). The final rule has significant implications for how health IT developers, health care providers and other stakeholders price access to application programming interfaces (APIs) and other technology used to access, exchange or use EHI. This On the Subject discusses the framework for determining whether license fees and other charges for use of such technology would comply with the final rule’s exceptions to the Cures Act’s information blocking prohibition and condition of certification for certified APIs.
On March 9, 2020, the Office of the National Coordinator for Health Information Technology (ONC) released its final rule under the 21st Century Cures Act to implement various policies to promote interoperability of health information technology (IT) and advance access, exchange or use of electronic health information (EHI) for continuity of care and other appropriate purposes. The final rule amends the certification requirements under the ONC Health IT Certification Program and identifies health IT pricing practices that do not fall under the Cures Act’s information blocking prohibition.
These final policies have significant implications for how certified health IT developers, health care providers, health information networks (HINs) and health information exchanges (HIEs) (collectively, actors) license and charge for technology to enable access, exchange or use of EHI with patients and other technology and service providers, health care providers and health plans.
Subject to limited exceptions, EHI covered by the information blocking prohibition includes electronic protected health information under the Health Insurance Portability and Accountability Act of 1996 (HIPAA) regulations (EPHI) to the extent that the EPHI is part of a patient’s electronic medical record or another designated record set under HIPAA, regardless of whether the records are used or maintained by or for a HIPAA covered entity. However, until the date 24 months after the publication of the final rule in the Federal Register, EHI is limited to the data elements represented in the US Core Data for Interoperability (USCDI) standard adopted under the health IT certification provisions of the final rule.
This On the Subject discusses the analytical framework for determining whether license fees and other charges for use of application programing interfaces (APIs) and other technology used to access, exchange or use EHI comply with the final rule’s information blocking exceptions and condition of certification for certified APIs. It also recommends practical next steps for implementing the final rule’s fee restrictions.
For more information about the final rule, including provisions that are not directly related to fees and other charges, see McDermott’s prior Special Report comprehensively covering the information blocking provisions of the final rule.
Does the information blocking prohibition restrict charges for health IT used to access, exchange and use EHI?
The final rule generally defines information blocking to mean a practice by an actor that is likely to interfere with, prevent or materially discourage access, exchange or use of EHI unless the practice is required by law or covered by an exception in the final rule. Because of this broad definition, any fees or other charges that an actor charges patients, health care providers, health plans, technology or service providers or other third parties for access, exchange or use of EHI or technology to enable such access, exchange or use, potentially implicate the information blocking prohibition. Consequently, those fees and charges, unless required by law, would need to fit within an information blocking exception to protect the actor from potential information blocking liability.
What information blocking exceptions protect licensee fees and other charges for use of health IT used to access, exchange and use EHI?
The final rule includes the following three exceptions for license fees and other charges for interoperability elements and other fees for use of technology that may interfere with EHI access, exchange or use. A fee or other charge that meets the definition of information blocking must satisfy at least one of these exceptions:
- Content and Manner Exception
- Fees Exception
- Licensing Exception
Content and Manner Exception
The Content and Manner Exception allows an actor and a party that requests EHI to negotiate mutually agreeable terms (including fees) for access, exchange and use of EHI. To be protected under the Content and Manner Exception, the actor must respond to a request for EHI with the subset of EHI identified by the USCDI data elements until the date 24 months after the publication of the final rule in the Federal Register. After that date, actors must respond with all EHI in a designated record set as discussed above.
In terms of the manner of response, an actor must fulfill a request for access, exchange or use of the required content in the manner requested, unless (1) the actor cannot technically fulfill the request, or (2) the actor and requestor are unable to reach mutually agreeable terms. If an actor fulfills a request in the manner requested, the limitations in the Fee Exception and Licensing Exception would not apply. Thus, the actor would have the opportunity to negotiate mutually agreeable fees and other terms with requestors.
If the actor does not fulfill a request in the requested manner, then the actor must fulfill the request in one of three alternative manners specified in the exception without unnecessary delay. When an actor fulfills a request in an alternative manner, the fees charged would have to meet the Fees Exception or the Licensing Exception.
Fees Exception
The Fees Exception allows an actor to charge fees, including those that result in a reasonable profit margin, for accessing, exchanging or using EHI, provided that the fee is:
- Based on objective and verifiable criteria, uniformly applied for similarly situated people/requests;
- Reasonably related to the actor’s costs;
- Reasonably allocated among all similarly situated people; and
- Based on costs not already recovered for the same instance of the service to a provider or third party.
In addition, the fee must not be based on:
- Competitive considerations;
- Sales, profit, revenue or other value that the requestor or other party may derive from the access, exchange or use of the EHI;
- Costs that an actor incurs because it designed or implemented health IT in non-standard ways (unless the requestor agreed to the fee associated with such implementation);
- Costs associated with intangible assets other than actual development and acquisition costs;
- Opportunity costs unrelated to the access, exchange or use of EHI; or
- Any costs leading to the creation of intellectual property if the actor charges a royalty for that intellectual property under the Licensing Exception and the royalty includes development costs of creating that intellectual property.
Additionally, an actor may not charge any of the following fees under the Fees Exception:
- Fees prohibited under the HIPAA Privacy Rule for individuals’ requests for access to their protected health information;
- Fees based in any way on the electronic access of an individual’s EHI by the individual, the individual’s personal representatives or others designated by the individual (The final rule defines “electronic access” as “an internet-based method that makes EHI available at the time the EHI is requested and where no manual effort is required to fulfill the request.” So whenever fulfilling individuals’ requests to send EHI to themselves or their personal representatives or others they designate, if the process requires manual effort, such as collating or assembling electronic health records from multiple systems, then the definition of electronic access would not be met and the actor could charge a fee and meet the Fees Exception.);
- Fees to export EHI to switch health IT or provide EHI to patients, if done through a capability certified to the final rule’s EHI export health IT certification criterion at 45 CFR § 170.315(b)(10) (Certified EHI Export Capability); and
- Fees to export or convert data from an EHR system, unless the parties agreed to the fee in writing at the time the EHR system was acquired.
In addition, this exception requires health IT developers that create certified API technology (certified API developers) to comply with the new condition of certification for certified APIs as a condition of meeting the Fees Exception.
Licensing Exception
Under the Licensing Exception, an actor’s terms (including those related to fees) for licensing an interoperability element for EHI to be accessed, exchanged or used is not prohibited information blocking when the practice meets all of the conditions discussed below. The final rule defines the term “interoperability element” to mean “hardware, software, integrated technologies or related licenses, technical information, privileges, rights, intellectual property, upgrades, or services that (1) may be necessary to access, exchange or use EHI and (2) are controlled by the actor. Such control includes the ability to confer all rights and authorizations necessary to use the element to enable the access, exchange or use of EHI.”
Upon receiving a request to license an interoperability element for the access, exchange or use of EHI, the actor must begin license negotiations with the requestor within 10 business days from receipt of the request and negotiate a license with the requestor, subject to the licensing conditions below (and other requirements of the Licensing Exception), within 30 business days from receipt of the request. The license for the interoperability element must meet the following conditions:
- Scope of Rights. The license must provide all rights necessary to: enable the access, exchange or use of EHI and to achieve the intended access, exchange or use of EHI via the interoperability element.
- Reasonable Royalty. If the actor charges a royalty for the use of the interoperability element, the royalty must be reasonable and comply with the following requirements:
- The royalty must be non-discriminatory, consistent with the non-discriminatory terms requirement below.
- The royalty must be based solely on the independent value of the actor’s technology to the licensee’s products, not on any strategic value stemming from the actor’s control over essential means of accessing, exchanging or using EHI.
- If the actor has licensed the interoperability element through a standards developing organization in accordance with its policies regarding the licensing of standards-essential technologies on terms consistent with the licensing exception, the actor may charge a royalty that is consistent with such policies.
- An actor may not charge a royalty for intellectual property if the actor recovered any development costs pursuant to the Fees Exception that led to the creation of the intellectual property.
In the final rule preamble, ONC notes that whether a royalty is reasonable for purposes of the Licensing Exception requirement depends on the particular facts and circumstances. ONC also identifies the following non-exclusive list of potential factors for evaluating reasonableness:
- The royalties received by the actor for the licensing of proprietary elements in other circumstances comparable to reasonable and non-discriminatory licensing circumstances.
- The rates paid by the licensee for the use of other comparable proprietary elements.
- The nature and scope of the license.
- The effect of the proprietary elements in promoting sales of other products of the licensee and the licensor, taking into account only the contribution of the elements themselves and not of the enhanced interoperability that they enable.
- The utility and advantages of the actor’s interoperability element over the existing technology, if any, that had been used to achieve a similar level of access, exchange or use of EHI.
- The elements’ contribution to the technical capabilities of the licensee’s products, taking into account only the value of the elements themselves and not the enhanced interoperability that they enable
- The portion of the profit or selling price that may be customary in the particular business or in comparable businesses to allow for the use of the proprietary elements or analogous elements that are also covered by reasonable and non-discriminatory terms commitments.
- The portion of the realizable profit that should be credited to the proprietary elements as distinguished from non-proprietary elements; the manufacturing process; business risks; significant features or improvements added by the licensee; or the strategic value resulting from the network effects, switching costs, or other effects of the adoption of the actor’s technology.
- The opinion testimony of qualified experts.
- The amount that a licensor and a licensee would have agreed upon (at the time the licensee began using the elements) if both were considering the reasonable and non-discriminatory terms obligation under the Licensing Exception and its purposes, and had been reasonably and voluntarily trying to reach an agreement.
- Non-Discriminatory Terms. The royalty and other terms on which the actor licenses and otherwise provides the interoperability element must be non-discriminatory and comply with the following requirements:
- The terms must be based on objective and verifiable criteria that are uniformly applied for all similarly situated classes of persons and requests.
- The terms must not be based in any part on:
- Whether the requestor or other person is a competitor or potential competitor, or will be using EHI obtained via the interoperability elements in a way that facilitates competition with the actor; or
- The revenue or other value the requestor may derive from access, exchange or use of EHI obtained via the interoperability elements.
Accordingly, the royalty or other compensation terms in the license agreement for the interoperability element may not be a revenue share based on the revenue that the licensee generates from EHI transferred through the interoperability element.
How does the condition of certification for APIs affect license fees and other charges?
ONC finalized a condition of certification for certified APIs that includes, among other requirements, restrictions on the pricing practices of certified API developers. The requirements directly applicable to the fee restrictions are as follows:
- Permitted Fees Generally. The condition of certification permits certified API developers to charge three categories of permitted fees and expressly allows the permitted fees to include a reasonable profit margin otherwise in accordance with the Fees Exception. All other fees related to certified API technology are prohibited. A certified API developer must ensure that:
- All permitted fees are based on objective and verifiable criteria that are uniformly applied to all similarly situated hospitals, physician practices and other organizations that deploy certified API technology (API information sources), and persons or entities that create or use software applications that interact with the certified API technology (API users).
- Permitted fees imposed on API information sources are reasonably related to the certified API developer’s costs to supply certified API technology to, and if applicable, support certified API technology for, API information sources.
- Permitted fees to supply and support certified API technology are reasonably allocated among all similarly situated API information sources.
- Fees are not based on whether API information sources or API users are competitors or potential competitors, or will use the API in a way that facilitates competition with the certified API developer.
- Three Categories of Permitted Fees. The condition of certification permits the following categories of fees for certified API technology:
- Permitted Fee: Development, Deployment and Upgrades. A certified API developer may charge fees to an API information source to recover the costs reasonably incurred by the certified API developer to develop, deploy and upgrade certified API technology.
- Permitted Fee: Recovering API Usage Costs. A certified API developer may charge fees to an API information source related to the use of certified API technology, provided that the fees are limited to the recovery of incremental costs reasonably incurred by the certified API developer when it hosts certified API technology for the health care provider or other API information source.
- Permitted Fee: Value-Added Services. A certified API developer may charge fees to an API user for value-added services related to certified API technology, as long as the services are not necessary to efficiently and effectively develop and deploy production-ready software that interacts with the certified API technology.
- Prohibited Fees. Consistent with the Fees Exception, the condition of certification prohibits a certified API developer from charging a fee for:
- Costs associated with intangible assets other than actual development or acquisition costs of such assets;
- Opportunity costs unrelated to the access, exchange or use of EHI; and
- Any costs that led to the creation of intellectual property if the actor charged a royalty for that intellectual property pursuant to the Licensing Exception and the royalty included the development costs for the creation of the intellectual property.
- Non-Discrimination. A certified API developer must meet the following non-discrimination requirements when setting fees and other terms with respect to certified API technology:
- Provide the certified API technology to an API information source on terms that are no less favorable than the certified API developer provides to itself and its own customers, suppliers, partners and other persons with whom it has a business relationship;
- Base the terms for the provision of certified API technology on objective and verifiable criteria that are uniformly applied to all substantially similar or similarly situated classes of persons and requests;
- Not offer different terms or services based on whether a competitive relationship exists or would be created; and
- Not offer different terms or services based on the revenue or other value that another party may receive from using the API technology.
- Description of API Fees. The certified API developer must describe all fees that it charges for the use of its certified API technology in detailed, plain language. The description must include all material information, including the persons or classes of persons to whom the fee applies; the circumstances in which the fee applies; and the amount of the fee, which for variable fees must include the specific variables and methodologies used to calculate the fee.
- Record-Keeping Requirements. A certified API developer must keep detailed records of any fees charged with respect to the certified API technology, the methodologies used to calculate the fees and the specific costs to which such fees are attributed. In the final rule preamble, the ONC states it expects that “the accounting practices already used by health IT developers will largely support the health IT developer to meet this requirement. Examples of these practices by health IT developers include the methods used to track their own investments, determine how to bill and issue invoices to their customers, document receipt of payment, and to maintain overall accurate financial records of business transactions.”
What is the analytical framework for determining whether charges for health IT comply with an information blocking exception under the final rule and, if applicable, the condition of certification for APIs?
If an entity desires to impose a fee or other charge for an interoperability element or EHI access, exchange or use, to the extent the information blocking prohibition applies, the entity must design the fee to meet an exception to the information blocking prohibition and any applicable conditions of certification for certified health IT, such as the restrictions on fees for certified APIs. Accordingly, the entity should consider the following questions:
- Covered Actor. Is the entity seeking to charge the license fees or other charges for use of APIs and other technology to access, exchange or use EHI an actor subject to the final rule (i.e., a health care provider, certified health IT developer, or an HIN or HIE)?
- EHI. Does the proposed fee or other charge relate to EHI, as opposed to HIPAA de-identified health information or other information outside the definition of EHI, such as (for the 24 months after the publication of the final rule in the Federal Register), information that is not included in the USCDI data set?
- Interoperability Element or Access, Exchange or Use. Is the proposed fee or other charge for (1) a license or other right to use an interoperability element or (2) providing access, exchange or use of EHI? For example, is the fee in exchange for a license for an API that enables access to EHI stored in an EHR system? Is the fee for a license to elements of EHR software or other health IT that only stores EHI rather than providing access, exchange or use of EHI? Alternatively, is the fee for participation in an HIN or HIE?
- Information Blocking Exception. Does the proposed fee or other charge meet the Content and Manner Exception, Fees Exception or Licensing Exception? The Content and Manner Exception provides the greatest flexibility for actors relative to pricing and terms and may, therefore, be the most advantageous exception for actors to consider first. Between the Licensing Exception and the Fees Exception, the Licensing Exception is typically more attractive if the applicable costs are low, so it may be advantageous to consider that exception before the Fees Exception.
- Additional Requirements for Certified API Technology. If the proposed fee or other charge relates to a certified API, does the proposed pricing practice meet the additional requirements of the condition of certification for APIs?
What are the key next steps for a certified health IT developer to ensure fees and other charges comply with the final rule’s information blocking prohibition and condition of certification for certified APIs?
A certified health IT developer should consider at least the following key steps to implement compliance.
- Step 1: Identify all executed and template contracts and other arrangements under which the developer provides technology that includes any capability or service that enables access, exchange or use of EHI to third parties rather than merely storing EHI.
- Step 2: Develop a business strategy and process for amending non-compliant arrangements with current customers and other counter-parties within the six-month period before the final rule’s compliance date for its information blocking provisions and for negotiating market terms with prospective counter-parties under the arrangements identified in Step 1 in accordance with the Content and Manner Exception.
- Step 3: Revise any template pricing terms that do not meet the restrictions of the Fees Exception or Licensing Exception in order to be prepared for the failure of negotiations of market terms in accordance with the Content and Manner Exception.
- Step 4: Develop a business process for responding to third-party requests to license an interoperability element, including its deadlines for beginning license negotiations and completing negotiations of a license agreement.
- Step 5: Ensure that any template license or other agreement with a new customer for an EHR system specifies any fees to export or convert data from the EHR system in order to avoid the prohibition on export and conversion fees that are not agreed to in writing at the time the EHR system is acquired.
- Step 6: Determine how to reasonably allocate certified API supply and support costs among similarly situated API information sources, including determining reasonably likely costs and forecasting the number of API information sources deploying the certified API.
- Step 7: Determine whether existing accounting practices maintain detailed records of fees charged with respect to the certified API and other technology, the methodologies used to calculate the fees and the specific costs to which such fees are attributed. If existing practices do not maintain detailed records of these items, establish a practical business process to attribute fees to costs and a record keeping system to track required information.
What are the key next steps for a health care provider (that is not a certified health IT developer) to ensure that its contracts and other arrangements comply with the fee restrictions in the final rule’s exceptions to the information blocking prohibition?
A hospital, physician practice or other health care provider actor should consider the following steps to implement compliance with the information blocking prohibition:
- Step 1: Identify all contracts and other arrangements under which the health care provider licenses or otherwise obtains an interoperability element or service from a certified health IT developer or other actor that enables access, exchange or use of EHI rather than merely storing EHI.
- Step 2: Evaluate the arrangements identified under Step 1 to determine whether any fees may fail to meet the limitations imposed under the applicable final rule exception, and if so, consider requesting modified pricing terms for non-compliant arrangements.
- Step 3: Develop a business strategy and process for responding to requests from physician practices and other health care provider requestors that have common patients with the health care provider receiving the request, for access, exchange or use of EHI maintained by the receiving health care provider. For example, a community physician practice may request that a hospital with common patients establish a custom interface to enable seamless access to EHI about common patients maintained by the hospital.
Summary Chart*
Our summary chart, available here, identifies all of the restrictions directly applicable to fees charged by an actor under the final rule. The first column of the chart identifies a restriction affecting fees. The second column indicates whether the fee restriction in the first column is an element of the Licensing Exception. The third column indicates whether the restriction in the first column is an element of the Fees Exception. The fourth column indicates whether the restriction applies to developers of certified APIs.
*For more information about elements of the exceptions that are not directly related to fees charged by an actor, please see McDermott’s prior Special Report comprehensively covering the information blocking provisions of the final rule.
Please do not hesitate to contact your regular McDermott lawyer or any one of the authors of this On the Subject if you have questions or need assistance with understanding the fee restrictions under the final rule.
For an in-depth discussion of the final rules and their impact on your organization, view the recordings of our March 2020 webinar series.
CMS Final Rule Aims to Advance Interoperability, Exchange of Clinical and Plan Information
CLIENT ALERT / INFORMATION BLOCKING / INTEROPERABILITY
March 16, 2020
Read time: 10 min
The Centers for Medicare & Medicaid Services (CMS) published its highly anticipated final rule aimed at enhancing interoperability and increasing patient access to health information. CMS’s final rule will require hospitals and payors to make significant investments in their health information technology to comply with the new requirements, effective six months following publication of the final rule in the Federal Register for hospitals, and January 1, 2021, for payors. In this On the Subject, we analyze the final rule requirements, which include a new requirement that CMS-regulated payors offer application programming interfaces, and a new Medicare condition of participation that requires hospitals with electronic health record systems to send electronic patient event notifications to communicate transitions of care.
On March 9, 2020, the US Department of Health and Human Services (HHS) Centers for Medicare & Medicaid Services (CMS) announced a final rule aimed at enhancing interoperability and increasing patient access to health information. The final rule requires CMS-regulated payors and agencies (Covered Plans and Agencies) to implement application programming interfaces (APIs) that allow patient information to be shared more readily between patients, healthcare providers, payors and third-party applications selected by patients. APIs could improve patients’ ability to gain access to their health information and share key medical history information with other providers and payors. Notably, however, HIPAA does not apply to many third-party applications that patients would use to access their data, raising stakeholder concerns about the privacy and security of information shared through APIs.
The final rule also requires hospitals that have adopted electronic health record systems to engage in electronic event reporting of patient admissions, discharges and transfers to patients’ primary care practitioners as a condition of participation (CoP) in the Medicare program. Hospitals and payors may need to make significant investments in health information technology (IT) to comply with the new requirements, which go into effect six months following publication of the final rule for hospitals, and on January 1, 2021, for payors.
This highly anticipated final rule has already garnered responses from key industry players, including America’s Health Insurance Plans, the nationwide association of health insurers, which stated that it shares HHS’s vision for expanded consumer data access but “remain[s] gravely concerned that patient privacy will still be at risk when health care information is transferred outside the protections of federal patient privacy laws.” The association cautioned that “any new rules must ensure we protect patient privacy, reduce health care costs, and get personalized information into the hands of patients.”
On the same day that CMS released the final rule, the HHS Office of the National Coordinator of Health IT (ONC) released a final rule implementing the information blocking provisions of the 21st Century Cures Act and updates to ONC’s health IT certification program. A separate On the Subject about the ONC final rule is forthcoming.
Read on for a summary of the key requirements and implications of the CMS final rule, and recommended next steps for payors and hospitals. For a review of our past coverage on these rules, please visit our Regulatory Sprint to Coordinated Care Resource Center.
Application Programming Interfaces
Under the final rule, Covered Plans and Agencies—which include Medicare Advantage (MA) plans, Medicaid state agencies, Medicaid managed care plans, Children’s Health Insurance Program (CHIP) agencies, CHIP Managed Care entities, and issuers of qualified health plans in federally facilitated exchanges, except for stand-alone dental plans—must adopt and implement an “openly published” API that permits third-party software applications to retrieve, at the direction of the patient or health plan member, a significant amount of clinical and payment information. The API technology must meet health IT standards established by ONC. Covered Plans and Agencies must comply by January 1, 2021.
The Covered Plan or Agency must make the following information available through the API:
- Data concerning adjudicated claims and encounter data, including claims data for payment decisions that may be appealed, were appealed, or are in the process of appeal, and provider remittances and enrollee cost-sharing pertaining to such claims
- Clinical data, including laboratory results, if the Covered Plan or Agency manages such data.
The Covered Plans and Agencies must make this information available no later than one business day after a claim is adjudicated or the Covered Plan or Agency receives the data.
For MA plans, Medicaid and CHIP fee-for-service programs, Medicaid managed care plans and CHIP managed care entities, the API must also allow access to a provider directory of the payor’s network of contracted providers, including names, addresses, phone numbers and specialties, updated no later than 30 calendar days after the payor receives the information or an update.
For MA organizations that offer Part D plans, the API must allow the third-party application to retrieve:
- Standardized data concerning adjudicated claims for covered Part D drugs, including remittances and enrollee cost-sharing, no later than one business day after a claim is adjudicated
- Pharmacy directory data, including the number, mix and addresses of network pharmacies
- Formulary data that includes covered Part D drugs and any tiered formulary structure or utilization management procedure that pertains to those drugs.
While the open API initiative in the final rule specifically applies to Covered Plans and Agencies, CMS also expressed the hope that other stakeholders, such as state-operated exchanges and private payors, will adopt similar requirements for access to information and interoperability so that even more patients can broadly access their health information and better manage care.
Payor-to-Payor Data Exchange
In addition to proposing payor-to-patient exchanges through APIs, CMS also finalized its proposal to require MA plans, Medicaid managed care plans, CHIP managed care entities and qualified health plan issuers on the federally facilitated exchanges to forward patient information maintained within the ONC-identified US Core Data Set for Interoperability to other payors designated by the requesting patient for up to five years after the patient has disenrolled from the plan (with the approval and direction of the patient). CMS anticipates that payors will leverage the API they put in place to comply with patient access requirements to additionally provide other payors access to the same data. CMS allows payors to use other methods of data exchange to accomplish this requirement, however. Covered Plans and Agencies must comply with the payor-to-payor exchange requirement by January 1, 2022.
Notably, CMS elected to not finalize its proposal to require Covered Plans and Agencies to participate in trusted health information exchange networks. CMS noted that although some commenters showed support for the proposal, other commenters noted the need for a mature Trusted Exchange Framework and Common Agreement (TEFCA), a set of policies and procedures for interoperable exchange, to be put in place first. ONC published a second draft TEFCA on April 19, 2019, but has not yet finalized it.
Hospital Condition of Participation
CMS finalized its proposal to adopt a Medicare hospital CoP that requires hospitals, psychiatric hospitals and critical access hospitals (CAHs) that have electronic event notification capabilities to send electronic notifications upon a patient’s admission, discharge or transfer to or from the hospital’s emergency department or inpatient service department. The CoP becomes effective six months after the final rule’s publication in the Federal Register.
CMS modified the CoP slightly from the proposed rule. The final CoP does not require hospitals to include diagnosis information within the notification. Instead, the notification must include at a minimum the patient’s name, treating practitioner name and sending institution name. The CoP does not require hospitals to send notifications to all providers that have an “established care relationship” with the patient, but only to the patient’s established primary care practitioner or other practitioner or practice group identified by the patient as primarily responsible for the patient’s care.
CMS stated that electronic patient event notifications, or automated electronic communications from discharging providers to another facility, could improve care coordination and potentially reduce readmissions by making a receiving provider aware of the care the patient has received elsewhere. However, this CoP creates a new set of requirements on top of existing Promoting Interoperability measures that CMS adopted to incentivize the use of health IT to improve care. Hospitals must already spend significant resources to achieve the Promoting Interoperability measures, and the new CoP requirement will likely increase hospitals’ overall compliance burden with respect to health IT implementation.
Information Blocking and Public Reporting
The final rule discourages clinicians from engaging in the practice of information blocking by requiring the public display, via an indicator on the Physician Compare website, of physicians and other clinicians who fail to attest as part of the CMS Merit-based Incentive Payment System (MIPS) program that they:
- Did not knowingly and willfully take action to limit or restrict the compatibility or interoperability of certified health IT
- Implemented technologies and practices to ensure that their certified health IT is connected and compliant with applicable law
- Responded in good faith and in a timely manner to requests to retrieve or exchange electronic health information.
Clinicians who fail to attest “yes” to the above statements would receive a potential reduction of Medicare reimbursement under MIPS, in addition to the negative indicator on the CMS Physician Compare website, which is available to patients who are seeking to compare Medicare-participating physicians and other clinicians.
CMS also requires eligible hospitals and CAHs to make “yes/no” attestations concerning their use of certified health IT in order to participate in the CMS Promoting Interoperability program. A hospital or CAH’s failure to attest “yes” will result in a negative indicator on a future CMS website that will display hospitals’ attestations under the Medicare Promoting Interoperability program.
CMS included these reporting requirements in the final rule to discourage hospitals and clinicians from engaging in information blocking. CMS expects to post the information for both clinicians and hospitals in late 2020.
Recommended Next Steps
The final rule will have a significant impact on Covered Plans and Agencies and hospitals. These entities should consider taking several practical steps in response to the final rule.
Recommendations for Covered Plans and Agencies
Covered Plans and Agencies should consider the following next steps in response to the final rule:
- Assess the technological capabilities of IT systems and quickly make any necessary adjustments to offer an API that is consistent with ONC standards
- Develop user guides or other resources that explain how a plan member or patient may obtain data through the API and protect their privacy by only selecting reputable third-party applications
- Work with other Covered Plans and Agencies to develop technical mechanisms and policy frameworks for connecting and sharing data in accordance with the payor-to-payor exchange requirement, which becomes effective in 2022.
Recommendations for Hospitals and CAHs
Given the aggressive timelines in the final rule, hospitals will soon need to assess the capabilities of existing IT systems and their readiness to send electronic notifications as required by the new CoP. Even with necessary systems in place, hospitals should review their intake and discharge workflows to ensure that they are consistently identifying the practitioner primarily responsible for patients admitted to the emergency and inpatient departments. To the extent that hospitals are not consistently capturing this information, they should consider revising their policies, procedures and training to emphasize the importance of obtaining the information, and should set up event notifications to the identified individual or group practice.
If you would like assistance in complying with any of the new requirements, please contact one of the authors or your regular McDermott lawyer.
Our experienced team, which includes several attorneys who previously worked at the US Department of Health & Human Services (HHS), has advised many clients on the potential impact of the HHS proposed rules on their businesses and has analyzed the final rules. We will host a series of webinars to discuss the final rules. Details are below and you may register by clicking here.
- March 23, 2020: ONC Final Information Blocking Rule
- March 26, 2020: CMS Interoperability Rule
- March 31, 2020: Navigating the New ONC Requirements for APIs
Analyzing ONC’s Proposed Rule: Fee Restrictions for Health IT and EHI
CLIENT ALERT / INFORMATION BLOCKING
March 26, 2019
Read time: 11 min
The ONC recently released a proposed rule under the 21st Century Cures Act to promote interoperability of health IT and advance access, exchange or use of electronic health information. If finalized, the proposed rule would have significant implications for how health IT developers, health care providers and other stakeholders price access to APIs and other technology used to access, exchange or use health information. This On the Subject discusses the proposed framework for determining whether license fees and other charges for such technology would comply with the ONC’s proposed exceptions to the Cures Act’s information blocking prohibition and proposed Condition of Certification for APIs.
On March 4, 2019, the Office of the National Coordinator for Health Information Technology (ONC) published in the Federal Register its proposed rule under the 21st Century Cures Act to implement various policies to promote interoperability of health information technology (IT) and advance access, exchange or use of electronic health information (EHI) for continuity of care and other appropriate purposes. The proposed rule would amend the certification requirements under the ONC Health IT Certification Program and identify health IT pricing practices that do not fall under the Cures Act’s information blocking prohibition.
These proposed policies would have significant implications for how certified health IT developers, health care providers, health information exchanges (HIEs) and health information networks (HINs) (collectively, Actors) charge for licenses to use application programming interfaces (APIs); for other Interoperability Elements (as defined below); and for access, exchange or use of EHI with patients and other technology suppliers, health care providers and health plans. This On the Subject discusses the analytical framework for determining whether license fees and other charges for APIs and other Interoperability Elements used to access, exchange or use EHI would comply with the proposed rule’s information blocking exceptions and Condition of Certification for APIs.
For more information about the proposed rule, see McDermott’s prior On the Subject or listen to our webinar on the proposed information blocking exceptions. The public may submit comments regarding the proposed rule until 5:00 pm EDT on May 3, 2019.
Does the Information Blocking Prohibition Restrict Charges for Health IT Used to Access, Exchange and Use EHI?
The proposed rule generally defines information blocking to mean a practice by an Actor that is likely to interfere with, prevent or materially discourage access, exchange or use of EHI unless the practice is required by law or covered by an exception adopted by ONC. ONC proposes to define EHI to include data that is electronic protected health information (EPHI) under the Health Insurance Portability and Accountability Act of 1996 (HIPAA) regulations, as well as other electronic individually identifiable health information.
Because of this broad definition of information blocking, any fees or other charges that an Actor charges patients, health care providers, health plans, technology suppliers or other third parties for access, exchange or use of EHI, or technology used for such access, exchange or use, potentially implicate the information blocking prohibition. In particular, ONC proposes that the information blocking prohibition apply to licensing Interoperability Elements, which are broadly defined to include all of the following:
- Any functional element of health IT, whether hardware or software, that could be used to access, exchange or use EHI for any purpose, including EHI transmitted by or maintained in disparate media, information systems, HIEs or HINs
- Any technical information that describes the functional elements of technology (such as a standard, specification, protocol, data model or schema) and that a person of ordinary skill in the art may require to use the functional elements of the technology, including for the purpose of developing compatible technologies that incorporate or use the functional elements
- Any technology or service that may be required to enable the use of a compatible technology in production environments, including but not limited to any system resource, technical infrastructure, or HIE or HIN element
- Any license, right or privilege that may be required to commercially offer and distribute compatible technologies and make them available for use in production environments
- Any other means by which EHI may be accessed, exchanged or used
ONC is likely to consider any pricing practice that involves an Interoperability Element as potentially interfering with access, exchange or use of EHI and, as such, potentially subject to the information blocking prohibition. Those practices, unless required by law, would need to fit within an information blocking exception.
What Information Blocking Exceptions Protect Licensee Fees and other Charges for Health IT Used to Access, Exchange and Use EHI?
The proposed rule includes the following exceptions for license fees and other charges for Interoperability Elements and other fees that may interfere with EHI access, exchange or use:
- Licensing of Interoperability Elements on Reasonable and Non-discriminatory Terms (Licensing Interoperability Element Exception)
- Exception for Recovering Costs Reasonably Incurred to Provide Access, Exchange or Use of EHI (Cost Recovery Exception)
A fee or other pricing practice that meets the definition of information blocking must satisfy at least one of these exceptions.
Licensing Interoperability Elements Exception
The proposed Licensing Interoperability Elements Exception would permit a certified health IT developer or other Actor to charge a fee for the use of an Interoperability Element that satisfies all of the restrictions of the proposed exception. The key restriction is that the Actor must base the fee solely on the independent value of the Actor’s technology to the licensee’s products. The fee must not be based on any strategic value stemming from the Actor’s control over essential means of accessing, exchanging or using EHI. Further, the Actor must not price the Interoperability Element based on the revenue or other value that the licensee may derive from access, exchange or use of EHI obtained via the Interoperability Elements, including the secondary use of EHI. A complete list of the restrictions directly applicable to the fees is available in the below chart.
This exception also requires health IT developers that are API Technology Suppliers to comply with a proposed new Condition of Certification when charging fees to API Data Suppliers or API Users (discussed further below).
- An API Technology Supplier is a health IT developer that creates the API technology that is presented for testing and certification to any of the certification criteria adopted or proposed for adoption at 45 CFR § 170.315(g)(7) through (g)(11).
- An API Data Provider is the organization that deploys the API technology created by the API Technology Supplier and provides access via the API technology to data it produces and electronically manages. In some cases, the API Data Provider may contract with the API Technology Supplier to perform the API deployment service on its behalf. However, in such circumstances, the API Data Provider retains control of what information is disclosed and how it is disclosed, and therefore for the purposes of this definition is considered to be the entity that deploys the API technology.
- An API User is a person or entity that uses or creates software applications that interact with the APIs developed by the API Technology Supplier and deployed by the API Data Provider. API Users include, but are not limited to, third-party software developers, developers of software applications used by API Data Providers, patients, health care providers, and payers that use apps or services that connect to API technology on their behalf.
Cost Recovery Exception
ONC proposes the Cost Recovery Exception to allow an Actor to recover the costs that it reasonably incurs to provide access, exchange or use of EHI plus a reasonable profit. As with the other exceptions, an Actor must comply with specific restrictions to meet the exception. For example, the pricing methodology used to recover the costs must be based on objective and verifiable criteria, uniformly applied for similarly situated people/requests; be reasonably related to the Actor’s costs; be reasonably allocated among relevant customers; not be based on competitive considerations; and not be based on sales, profit, revenue or other value that the requestor or other party may derive from the access, exchange or use (including secondary use) that exceeds the Actor’s reasonable costs for providing such access, exchange or use of EHI.
Additionally, ONC would explicitly exclude certain costs from protection under the exception such as the following:
- Fees prohibited under the HIPAA Privacy Rule for individuals’ requests for access to their protected health information
- Fees based in any way on electronic access by individuals (or their personal representatives, agents or designees) to the individual’s EHI
- Fees to export EHI to switch health IT or provide EHI to patients, if done through a capability certified to the new certification criterion concerning EHI export capability (discussed below)
- Fees to export or convert data from an EHR, unless the parties had agreed to the fee at the time the EHR was acquired
The below chart includes a complete list of the specifically excluded costs, as well as other restrictions directly affecting pricing.
Like the Licensing Interoperability Elements Exception, this exception requires API Technology Suppliers to comply with proposed new conditions of certification for certified APIs. This exception also imposes the API Condition of Certification fee restrictions on API Data Providers.
How does the proposed Condition of Certification for APIs affect license fees and other charges?
ONC proposes to adopt a Condition of Certification for APIs that restricts the pricing practices of certified health IT developers that are API Technology Suppliers. The Condition of Certification limits API Technology Suppliers to charging fees that fall into one of three categories:
- Fees to recover reasonably incurred development, deployment and upgrade costs
- Fees to recover reasonably incurred incremental costs for supporting use of the API for purposes other than patient access, subject to certain limitations
- Fees for value-added services supplied in connection with software that can interact with the API as long as those services are not necessary to develop or deploy the software
Under the Condition of Certification, all fees charged by an API Technology Supplier must also meet general conditions aimed at ensuring that the fees are based on objective and verifiable criteria that are uniformly applied; are reasonably related to the API Technology Supplier’s costs, which must be reasonably allocated among all relevant customers; and are not based on competitive considerations. A complete list of the conditions applicable to pricing practices is included in the below chart.
As noted above, the Cost Recovery Exception to the information blocking prohibition would also impose the API Conditions of Certification fee limitations on an API Data Provider (e.g., a hospital that licenses EHR software with an API), even if the API Data Provider is not a certified health IT developer.
What is the Analytical Framework for Determining Whether Charges for Health IT comply with an information blocking exception under the proposed rule and, if applicable, the Condition of Certification for APIs?
If an Actor desires to impose a fee or other charge for an Interoperability Element or EHI access, exchange or use, it must design the fee to meet an exception to the information blocking prohibition and any applicable conditions of certification for certified health IT, such as the restrictions on fees for certified APIs. Accordingly, the Actor should consider the following questions:
- EHI. Does the proposed fee or other charge relate to EHI, as opposed to HIPAA de-identified health information or other information outside the definition of EHI?
- Technology or Practice. Is the proposed fee or other charge for a license or other right to use an Interoperability Element, or for providing access, exchange or use of EHI? For example, is the fee in exchange for a license for an API that enables access to EHI stored in an EHR system? Alternatively, is the fee for a license to elements of EHR software or other health IT that stores EHI rather than providing access, exchange or use of EHI?
- Information Blocking Exception. Does the proposed pricing practice meet either the Interoperability Element Exception or the Cost Recovery Exception? The Interoperability Element Exception is typically more attractive if the applicable costs are low, so it may be advantageous to consider that exception first.
- Additional Requirements for Certified APIs. If the proposed fee relates to a certified API, does the proposed pricing practice meet the additional Condition of Certification for APIs?
The following chart identifies all of the restrictions directly applicable to fees charged by an Actor under the proposed rule. The first column of the chart identifies a restriction affecting fees. The second column indicates whether the restriction in the first column is an element of the Licensing Interoperability Element Exception. The third column indicates whether the restriction in the first column is an element of the Cost Recovery Exception. The fourth column indicates whether the restriction applies to certified APIs.
Capitalized terms used in the chart have the meanings given to them by the proposed rule or the HIPAA administrative simplification regulations.
Click here or select the image to view the full chart.
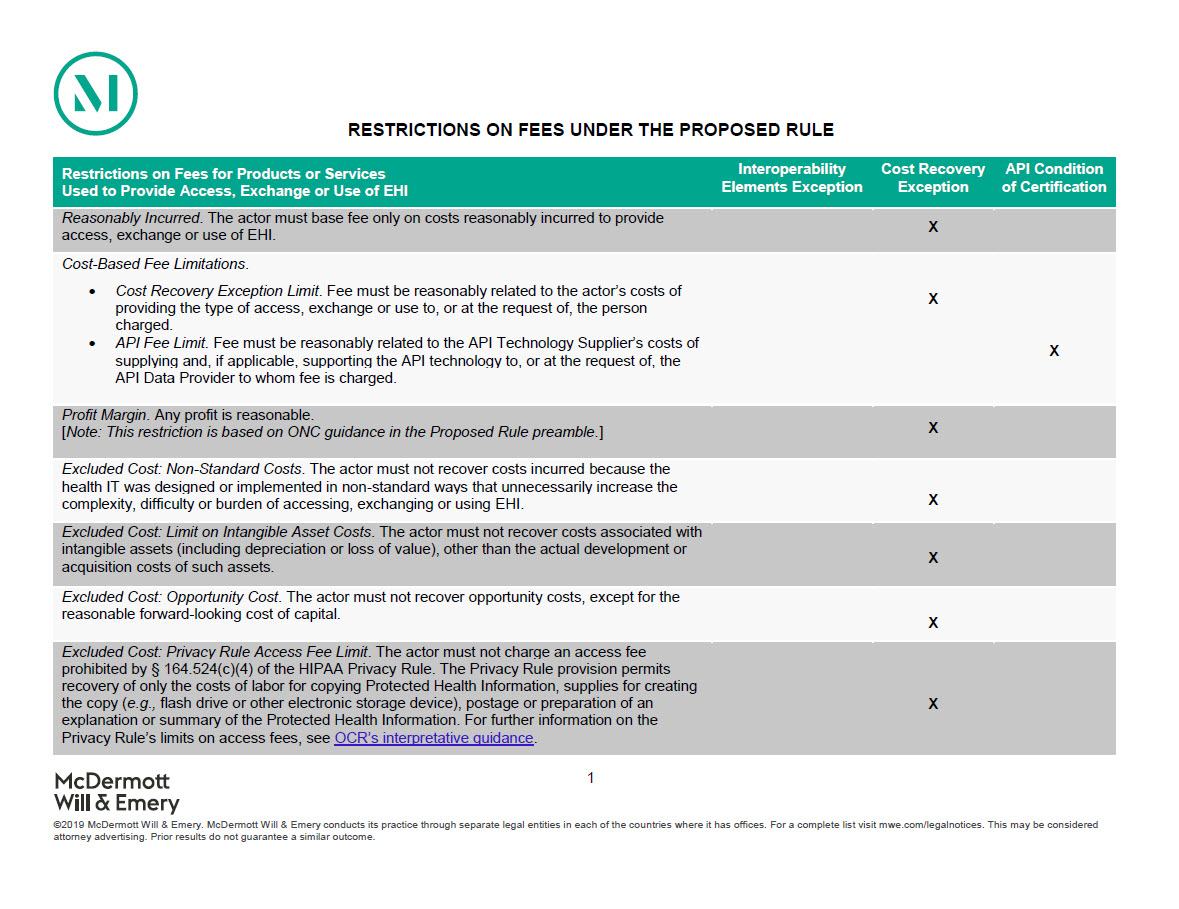

ONC Proposes to Define Conduct That Is Not Information Blocking under the Cures Act
CLIENT ALERT / INFORMATION BLOCKING
February 14, 2019
Read time: 19 min
The ONC finally released its long-awaited proposed rule to implement the “information blocking” prohibition of the 21st Century Cures Act by identifying conduct that is not information blocking. If finalized, ONC’s proposed rule would have a significant impact on data sharing arrangements and other relationships among health care providers, health IT developers and other stakeholders. In this On the Subject, our experienced team analyzes ONC’s information blocking proposals and suggests practical next steps for the regulated industry.
This On the Subject was co-authored by Rachel Stauffer at McDermott+Consulting
Summary
On February 11, 2019, the Office of the National Coordinator for Health Information Technology (ONC) released its long-awaited proposed rule (Proposed Rule) that, among other things, proposes to implement the “information blocking” prohibition of the 21st Century Cures Act (the Cures Act) by identifying conduct that is not information blocking. On the same day, the Centers for Medicare and Medicaid Services (CMS) released a proposed rule on related interoperability issues. We cover the CMS proposed rule in a separate On the Subject. If finalized, ONC’s proposed policies would have a significant impact on data sharing arrangements and other relationships among health care providers, health IT developers and other stakeholders.
More broadly, these two rules emphasize the administration’s focus on ensuring patient access to data and data exchange. As CMS Administrator Seema Verma recently explained, “[t]he days of holding patient data hostage are over…Our proposed rule includes a policy to publicly identify doctors, hospitals, and other healthcare providers who engage in information blocking. Simply put, we’re going to expose the bad actors who are purposely trying to keep patients from their own information. Patient data doesn’t belong to the doctor, hospital, or electronic health record. It belongs to the patient.” ONC’s Proposed Rule reflects a similar sentiment.
The public will have 60 days to submit comments following official publication of the Proposed Rule in the Federal Register, which we expect to occur in the near future.
The following sections of this On the Subject address:
- The events leading up to the adoption of the Cures Act and the Proposed Rule;
- Discussion and analysis of the information blocking provisions of the Proposed Rule, including its exceptions describing permissible conduct under the Proposed Rule; and
- Practical impact and next steps for health care industry stakeholders.
A. Background
Since passage of the Health Information Technology for Economic and Clinical Health Act in 2009, the federal government has invested billions of dollars to encourage the adoption of interoperable technologies in the hope that it will lead to better care and a more efficient health care system. Congress, regulators and health care industry stakeholders, have grown concerned that, despite increased adoption of technology, like electronic health record (EHR) systems, certain economic and market conditions create an incentive for some to inappropriately limit or restrict the flow of electronic health information in ways that undermine the significant investment; this conduct is commonly referred to as “information blocking.”

OCR Explains How Information Blocking Violates HIPAA
CLIENT ALERT / INFORMATION BLOCKING
October 26, 2016
Read time: 5 min
The US Department of Health and Human Services Office for Civil Rights recently posted guidance clarifying that a business associate such as an information technology vendor generally may not block or terminate access by a covered entity customer to protected health information maintained by the vendor on behalf of the customer.
The US Department of Health and Human Services (HHS) Office for Civil Rights (OCR) recently posted guidance (OCR guidance) clarifying that a business associate such as an information technology vendor generally may not block or terminate access by a covered entity customer to protected health information (PHI) maintained by the vendor on behalf of the customer. Such “information blocking” could occur, for example, during a contract dispute in which a vendor terminates customer access or activates a “kill switch” that renders an information system containing PHI inaccessible to the customer. Many information vendors have historically taken such an approach to commercial disputes.
The OCR guidance explains that such activity by a business associate is an impermissible use of PHI in violation of the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule. In addition, to the extent the PHI constitutes a designated record set, such activity could cause a vendor to violate its obligations under the applicable business associate agreement and the Privacy Rule to make available PHI to a customer as necessary for the customer to satisfy its obligation to provide access to PHI to individuals under the Privacy Rule.
A business associate is also required by the HIPAA Security Rule to ensure the confidentiality, integrity and availability of PHI that it creates, receives, maintains or transmits on behalf of a covered entity. Under HIPAA, “availability” means that data or information is accessible and useable upon demand by an authorized person. A vendor that blocks a covered entity customer’s access to essential PHI potentially violates the Security Rule’s “availability” requirement.
Moreover, the OCR guidance clarifies that maintaining the availability of PHI includes returning PHI at the termination of an agreement to a customer in a format that is reasonable in light of the vendor’s obligations under a business associate agreement. OCR acknowledged, however, that not all arrangements involving PHI require the covered entity to be able to access PHI. For example, some data aggregation arrangements will not implicate the information blocking prohibition when the source data that is used to create the aggregated data set is unreturnable after the data processing.
Finally, the OCR guidance notes that a covered entity itself has an obligation to ensure the availability of its own information and may be in violation of both the Privacy Rule and the Security Rule provisions relating to business associate arrangements if it enters into a business associate agreement that by its terms prevents the covered entity from fulfilling this obligation. This new guidance should serve as reminder to covered entities to take care in drafting and negotiating business associate agreements and service agreements to protect against information blocking.
The OCR guidance would not prevent a vendor from charging a fee for access to or post-termination transfer of a covered entity’s data, the amount of which would be primarily a contractual matter. Instead, OCR has taken the position in the guidance that blocking access to PHI is not an appropriate remedy for non-payment of fees or other contractual disputes.
The OCR guidance adds to previous HHS activity discussing information blocking as a barrier to interoperability and health information exchange and a potential source of liability under the federal Anti-Kickback Statute, including the following:
- In April 2015, HHS’s Office of the National Coordinator for Health Information Technology (ONC) submitted a Report on Health Information Blocking to the US Congress that defined “information blocking” as the knowing and unreasonable interference with the exchange or use of electronic health information. The report outlined a number of scenarios that describe information blocking conduct, including an electronic medical record (EHR) system billing dispute that results in the termination of customer access to PHI.
- On October 6, 2015, the HHS Office of Inspector General (OIG) issued an OIG Policy Reminder: Information Blocking and the Federal Anti-Kickback Statute (OIG Policy Reminder) that reminds health care providers that a safe harbor to the federal Anti-Kickback Statute related to the provision of EHR technology requires that a donor of EHR technology must not take any action to limit or restrict the use, compatibility, or interoperability of the items or services with other electronic prescribing or EHR systems (including, but not limited to, health information technology applications, products, or services).
In February of this year, HHS announced that health information technology developers whose products cover 90 percent of the country’s electronic health records and five largest health care systems agreed to implement a commitment to refrain from engaging in information blocking as part of its voluntary Interoperability Pledge.

